
Laparoscopy for Infertility in India: Tubal Recanalization, Hysteroscopy & Endometriosis Treatment for Australian, UK & Nigerian Patients
In India,
laparoscopy for infertility usually costs around ₹70,000 to ₹1,80,000 (about
$850–$2,200 or £680–£1,750) in well-equipped, accredited fertility centres.
Compared to places like the UK or Australia, this is often much cheaper —
sometimes 60–75% less. For patients from countries like Nigeria, it can also be
difficult to find advanced infertility laparoscopy locally, since only a few
centres offer it. That’s why many people look toward India, where the procedure
is more widely available, done by experienced specialists, and includes
structured post-surgery care at a lower overall cost.
This guide covers what laparoscopy for infertility
involves and how it compares to hysteroscopy. It covers tubal recanalization
procedure types and costs, as well as endometriosis and fertility outcomes.
Success rate data comes from peer-reviewed literature and NABH-accredited
partner hospitals.
What Is Laparoscopy for
Infertility and When Is It Recommended?
How Laparoscopy Works and What It
Can Treat
Laparoscopy for
infertility is a minimally invasive surgical procedure. A thin, lighted
telescope — the laparoscope — is inserted through a small incision near the
navel. Carbon dioxide gas expands the abdominal cavity. This gives the surgeon
a clear view of the pelvis, fallopian tubes, ovaries, and the outer surface of
the uterus. Instruments inserted through 1–2 additional small incisions allow
simultaneous treatment in the same session.
Laparoscopy for
infertility can diagnose and treat endometriosis, pelvic adhesions, fallopian
tube blockages, ovarian cysts, and uterine fibroids. It also treats PCOS via
ovarian drilling. It can also treat polycystic ovary syndrome (PCOS) via
ovarian drilling. A 2022 JBRA Assisted Reproduction review (Arab et al.) found that
diagnostic laparoscopy identifies pathology in approximately 40% of
‘unexplained infertility’ patients. That means one in four ‘unexplained’ cases
has a treatable cause only visible at laparoscopy.
When Do Doctors Recommend
Laparoscopy for Infertility?
Fertility
specialists typically recommend laparoscopy when:
•
In
cases of unexplained infertility—where a couple has been trying for 12 months
or more, semen analysis is normal, and the fallopian tubes appear open on
HSG—laparoscopy can still reveal hidden problems. Studies suggest that around
40% of these cases show some underlying pathology during laparoscopy (Arab et
al., JBRA, 2022).
•
Suspected endometriosis — pelvic pain, painful
periods, or deep pain with intercourse that hasn’t been explained by an
ultrasound
•
Abnormal HSG (hysterosalpingogram) — suggesting
tubal blockage or pelvic adhesions
•
Recurrent miscarriage — to check for pelvic or
uterine structural factors
•
PCOS unresponsive to ovulation induction
medications — ovarian drilling via laparoscopy is an alternative
•
Before IVF, in specific cases — to improve
uterine receptivity by treating endometriosis or fibroids
What Are the Disadvantages of
Laparoscopy?
Laparoscopy is
generally safe at accredited centres, but risks include:
•
General anaesthesia risk — rare but not zero;
full pre-operative assessment is standard at NABH/JCI-accredited hospitals
•
Mild
shoulder tip pain for a day or two after a laparoscopy is normal. It’s caused
by the gas used during surgery irritating the diaphragm. It usually goes away
quickly with movement and basic pain relief.
•
Bleeding
or infection at the incision sites is uncommon after laparoscopy. If it
happens, it is usually mild and can be managed with routine post-operative care
and basic treatment.
•
Rare
visceral injury — Injury to nearby organs such as the bowel, bladder, or major
blood vessels is very rare, occurring in less than 0.5% of cases at accredited
centres based on published surgical safety data.
•
Incomplete treatment — complex endometriosis or
extensive adhesions may require staged procedures.
•
Anaesthesia not feasible for some patients —
severe cardiac or respiratory conditions may preclude general anaesthesia.
At NABH-accredited hospitals like
Apollo Chennai, Fortis Noida, Medanta Gurugram, and Max Hospitals, pre-operative
checks are done following ICMR guidelines. International patients are also
clearly informed about the risks and what to expect during the consultation
before the procedure.
Endometriosis and
Fertility: How Laparoscopy Treats the Most Common Cause
Endometriosis
is the most common surgically treatable cause of infertility. It is found in
25–50% of women investigated for infertility and in 40% of women with chronic
pelvic pain. (ASRM Practice Committee, Fertility and Sterility, 2014.)
Laparoscopy is both the gold standard for diagnosis and the primary surgical
treatment.
Can a Woman with Endometriosis
Get Pregnant?
Yes — but the
probability depends on the stage. Women with Stage I or II endometriosis
(minimal to mild disease) have monthly conception rates of approximately 2–4%
naturally. This compares with 15–20% in women without the condition (ASRM
data). Surgical treatment of Stage I/II endometriosis via laparoscopy improves
monthly fecundity rates by approximately 1.6-fold per the Endocan trial. Women
with Stage III/IV endometriosis have lower untreated pregnancy rates. They
benefit more from combined surgery plus IVF.
How Does Endometriosis Affect
Infertility?
Endometriosis can reduce fertility in
a few different ways. First, the inflammation from active disease can affect
egg quality and also make it harder for sperm to move normally. Second, as the
condition heals, it can leave behind scar tissue (adhesions) that may pull or
distort the tubes and ovaries, making it difficult for the egg to be picked up.
Third, it can form ovarian cysts called endometriomas, which can gradually
reduce ovarian reserve. And finally, it may also affect the immune environment
inside the uterus, which can interfere with implantation—even when the embryo
is genetically normal and healthy.
Around 30–50% of women with
endometriosis may face fertility issues (Zondervan et al., Nature Reviews
Disease Primers, 2018). What’s important is that it doesn’t always depend on
how advanced the disease is. Even mild or early-stage endometriosis (Stage I)
can affect fertility, mainly because of inflammation and changes in the immune
environment, rather than visible structural damage.
Will Removing Endometriosis
Increase Chances of Conceiving?
Yes, for Stages I
and II, the evidence is clear. The Endocan study (Marcoux et al., NEJM, 1997)
found laparoscopic treatment of minimal-to-mild endometriosis roughly doubled
pregnancy rates at 36 weeks — compared with diagnostic laparoscopy alone. This
was compared with diagnostic laparoscopy alone. For Stage III/IV, surgical
excision reduces pain and improves quality of life. The fertility benefit is
less consistent and depends on ovarian reserve and remaining tubal function.
Most fertility specialists recommend an IVF consultation after Stage III/IV laparoscopy
rather than waiting for natural conception.
At centres like Apollo Chennai and
Medanta Gurugram, post-surgery care is not just about recovery. Before leaving
the hospital, patients are usually given a clear next-step plan—how long to try
for natural conception, when IVF may be considered if needed, and how ovarian
reserve will be monitored through follow-up tests.
What Age Is Best to Get Pregnant
with Endometriosis?
For women with
endometriosis, the general clinical recommendation is to pursue pregnancy
sooner rather than later. Endometriosis is a progressive condition. Lesions
tend to recur after surgical excision, and the window of improved fertility
after surgery is finite. Most fertility specialists recommend actively trying
to conceive within 6 months of laparoscopic excision. For women under 35 with
Stage I/II endometriosis and normal ovarian reserve, natural conception within
6–12 months of surgery is realistic. For women over 35 or with Stage III/IV
disease, concurrent fertility planning is typically discussed at the same
pre-operative consultation. This includes IVF.
What Percentage of People with
Endometriosis Are Infertile?
About 30–50% of women with
endometriosis may struggle to conceive (Zondervan et al., Nature Reviews
Disease Primers, 2018). At the same time, endometriosis is found quite often
during infertility evaluations—roughly in 25–50% of cases.
It works both ways—some women with
endometriosis have trouble conceiving, and many women being investigated for
infertility are later diagnosed with endometriosis. What’s not always obvious
is that the fertility impact doesn’t depend only on how “severe” it looks. Even
early or mild endometriosis can still affect fertility, mainly due to
inflammation and subtle changes in the pelvic environment that don’t show up
clearly on routine tests.
Laparoscopy vs
Hysteroscopy: Which Is Better for Infertility?
Laparoscopy
and hysteroscopy examine different anatomical spaces and are not
interchangeable. They are complementary rather than competing procedures. The
table below compares the two.
|
Feature |
Laparoscopy |
Hysteroscopy |
Anaesthesia |
Recovery |
Best
For |
|
Area |
Abdomen
& pelvis — external uterus, tubes, ovaries |
Uterine
cavity — internal lining |
General |
1–2
wks |
Endometriosis,
adhesions, tubal blockage, ovarian cysts |
|
Access |
Small
abdominal incision (keyhole) |
Through
the cervix — no incision |
Local
or general |
1–2
days |
Polyps,
fibroids, septum, intrauterine adhesions (Asherman’s) |
|
Hospital
stay |
Day
surgery or 1 night |
Day
surgery |
— |
— |
Can
be combined in one session (‘pan-endoscopy’) |
|
Treats |
Diagnoses
+ treats in same session (if operative) |
Diagnoses
+ treats in same session |
— |
— |
Combine
when both pelvic and uterine causes are suspected |
Sources:
This is based on established
ICMR ART guidelines and ASRM Practice Committee recommendations, as well as
standard protocols followed at leading partner hospitals such as Apollo
Chennai, Fortis Noida, Medanta Gurugram, and Max Hospitals. Care decisions
follow evidence-based clinical pathways.
What Is Hysteroscopy and When Is
It Recommended?
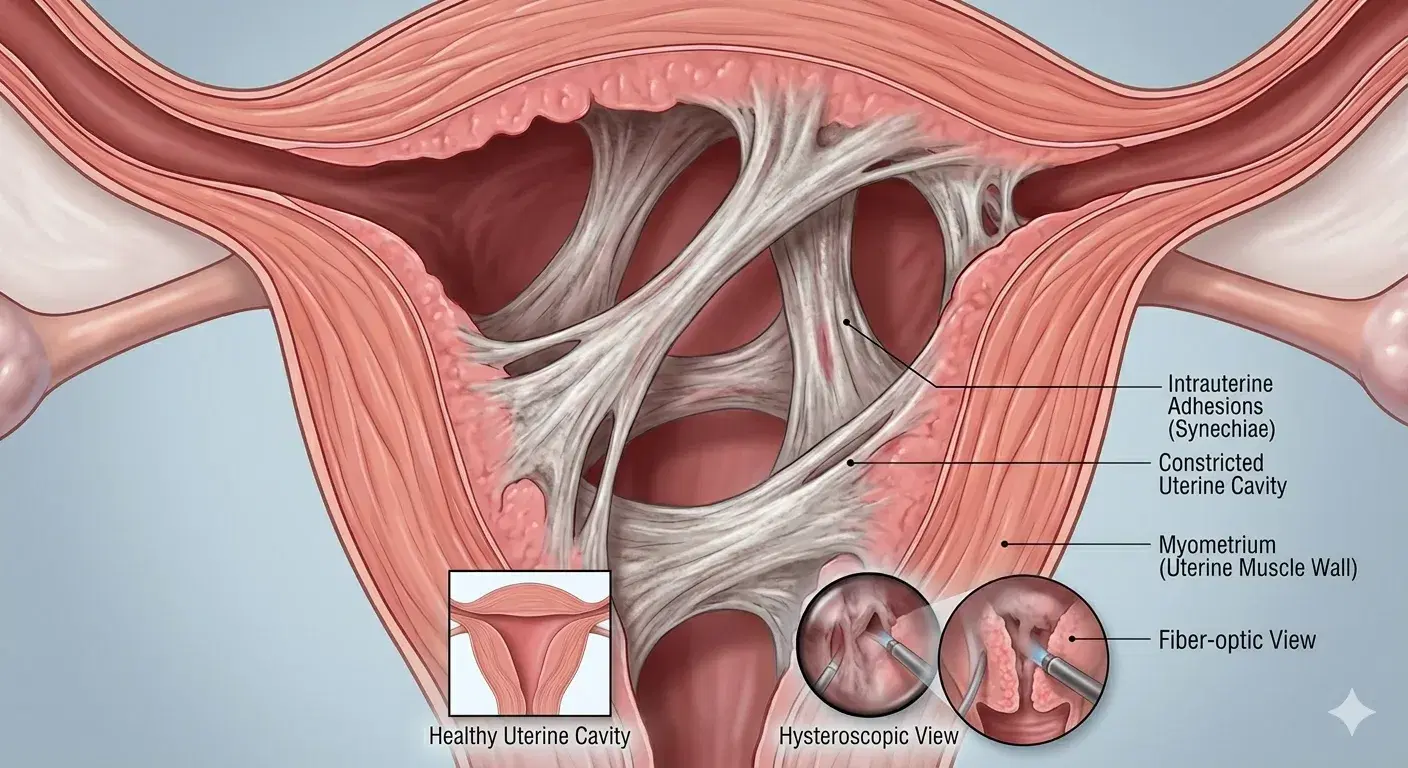
Hysteroscopy
directly visualises the inside of the uterine cavity. A thin telescope is
inserted through the cervix — no incision is needed. It diagnoses and treats
conditions inside the uterus: endometrial polyps, submucosal fibroids, uterine
septum, intrauterine adhesions, and chronic endometritis. These are conditions
that impair embryo implantation rather than egg transport.
Hysteroscopy is
recommended when an ultrasound suggests an intrauterine abnormality. It is also
recommended for recurrent implantation failure in IVF. A filling defect shown
on a hysterosalpingogram is another indication. At Fortis Noida and MAX
Hospitals, hysteroscopy is an outpatient day surgery. It is performed under
local or light general anaesthesia with same-day discharge.
Which Is Better — Hysteroscopy or
Laparoscopy?
Neither is
universally better — the right procedure depends on where the fertility problem
is located. If the suspected issue is outside the uterus (endometriosis,
blocked tubes, pelvic adhesions, ovarian cysts), laparoscopy is required. If
the suspected issue is inside the uterus (polyps, fibroids, scarring, septum),
hysteroscopy is required. When both are possible, a combined session — called a
pan-endoscopy — addresses both in a single anaesthetic.
Hysteroscopy is
faster, does not require abdominal incisions, and has a 1–2 day recovery.
Laparoscopy has a 1–2 week recovery and requires general anaesthesia. For
international patients, the combined approach is often the most efficient use of
the India trip. Both investigations are completed in one session.
Can Laparoscopy and Hysteroscopy
Be Done at the Same Time?
Yes. Performing
both procedures in a single surgical session is standard practice at
NABH-accredited fertility hospitals in India. This ‘pan-endoscopy’ approach
provides a complete picture of both the uterine cavity and the pelvic organs
under a single anaesthetic. Recovery is the same as laparoscopy alone — 1–2
weeks. The combined cost in India is ₹1,00,000–₹2,50,000 ($1,200–$3,000). In
Australia or the UK, separate procedures each require individual hospital
admissions and anaesthetics.
Tubal Recanalization for
Fallopian Tube Blockages
Tubal
recanalization is the general term for procedures that restore patency to
blocked fallopian tubes. Two fundamentally different procedures carry this
label — one is a radiology-guided outpatient procedure, the other is microsurgery.
Understanding the difference is critical because they have different
indications, costs, recovery times, and success rates.
Selective Salpingography + Tubal
Cannulation vs Microsurgical Reversal
|
Procedure
Type |
India Cost |
Duration |
Best For |
|
Selective
Salpingography + Tubal Cannulation (radiological — catheter-based) |
₹30,000–₹60,000
($360–$720; £290–£570) |
30–60 min,
outpatient, no GA |
Proximal tubal
blockage (near the uterus) caused by a mucus plug or debris. No surgery
needed. |
|
Microsurgical
Tubal Reversal (surgical — laparoscopic or open) |
₹1,50,000–₹3,50,000
($1,800–$4,200; £1,430–£3,330) |
2–4 hrs, 1–2
night stay, GA |
Tubal ligation reversal;
longer-segment blockage. Restores natural conception for multiple future
pregnancies. |
Sources: ICMR clinical
guidelines; partner hospital procedure data. Costs are approximate
private-patient rates at NABH-accredited facilities in Delhi NCR and Chennai.
The FAQ on this
blog — and most blogs — use ‘tubal recanalization’ without specifying which
type. When you contact a clinic, always clarify which procedure they mean.
Selective salpingography is catheter-based, outpatient, and lower cost.
Microsurgical reversal involves an operating theatre, general anaesthesia, and a
higher cost. Most patients with post-infective proximal tubal blockage need the
catheter-based procedure. Most patients who’ve had a sterilisation and now want
fertility restored need microsurgical reversal.
Who Is a Good Candidate for Tubal
Recanalization?
For selective
salpingography (radiological): good candidates have proximal fallopian tube
blockage confirmed by HSG. The blockage should be caused by debris, mucus
plugging, or mild scarring from past infection. The rest of the tube must be
healthy. Recurrence of blockage after the procedure is possible (approximately
15–30%), so patients should try to conceive promptly.
Microsurgical
tubal reversal: good candidates are women who have had a tubal ligation and now
want to conceive naturally. Age is critical. Women under 38 with at least 4–5
cm of healthy remaining tube have the best outcomes. Pregnancy rates are 50–80%
within 2 years. Women over 40 or with less than 4 cm of remaining tube are
typically better served by IVF.
Is Fallopian Tube Recanalization
the Same as HSG?
No — they are
different procedures. An HSG (hysterosalpingography) is a diagnostic X-ray.
Contrast dye is injected through the cervix into the uterus and fallopian
tubes. X-ray imaging shows whether the tubes are open or blocked. It diagnoses
blockages but does not treat them. Selective salpingography + tubal cannulation
is the therapeutic procedure that clears the blockage. A catheter is guided
through the cervix under fluoroscopy. If an HSG identifies a proximal blockage,
the cannulation procedure can sometimes be performed in the same radiology
session.
Signs of Pregnancy After Tubal
Recanalization
Signs of
pregnancy after tubal recanalization are the same as any natural pregnancy.
These include a missed period, nausea, breast tenderness, and a positive hCG
test. The key point is that tubal recanalization carries an elevated risk of
ectopic pregnancy. The risk is 2–5% for selective salpingography and 4–8% for
microsurgical reversal — higher than natural conception. Every positive
pregnancy test after either procedure must be confirmed by ultrasound at 6–7
weeks. This verifies the pregnancy is inside the uterus. One-sided lower
abdominal pain, shoulder tip pain, or unusual bleeding alongside a positive
test is a medical emergency. Seek care immediately.
Success Rates for Laparoscopy
and Tubal Recanalization
The table below gives an overview of
natural pregnancy rates after laparoscopic surgery and tubal recanalization at
NABH-accredited fertility centres in India. The results are broadly consistent
with internationally published benchmarks.
|
Condition
/ Procedure |
Natural
Pregnancy Rate |
Timeframe |
Notes |
|
Mild-to-moderate
endometriosis (laparoscopic excision) |
40–60% |
1–2
years |
Operative
laparoscopy outperforms diagnostic-only, stage I/II |
|
Pelvic
adhesions (adhesiolysis via laparoscopy) |
30–50% |
1–2
years |
Outcomes
depend on tubal patency after adhesiolysis |
|
Proximal
tubal blockage (selective salpingography) |
20–40% |
6–12
months |
Ectopic
pregnancy risk 2–5%; early ultrasound mandatory |
|
Tubal
ligation reversal (microsurgical) |
50–80% |
1–2
years |
Best
outcomes: women under 38, ≥4 cm healthy tube remaining |
|
Ovarian
drilling (PCOS-related anovulation) |
40–60% |
6–12
months |
Alternative
to ovulation induction medications |
Sources:
These references include Arab W et al. (JBRA Assisted Reproduction,
2022) on laparoscopy in unexplained infertility, ASRM Practice Committee
Guidelines on endometriosis (Fertility and Sterility, 2014), and Marcoux et al.
(NEJM, 1997) on endometriosis excision outcomes. It also draws on outcome
experience from partner hospitals such as Apollo Chennai, Fortis Noida, Medanta
Gurugram, and Max Hospitals. All figures refer to natural pregnancy rates over
the stated timeframes. Individual results can vary depending on age, ovarian
reserve, male factor fertility, and the extent of disease.
Laparoscopy mainly helps by treating
problems that can make natural conception difficult, like inflammation,
endometriosis, or structural issues. But it doesn’t replace IVF when there are
other factors involved, such as low sperm count, reduced ovarian reserve, or
age-related fertility decline. In those situations, IVF may still be needed.
After surgery, the doctor looks at your overall reports and guides you on what
makes more sense next—trying naturally for some time or going ahead with IVF
Is Laparoscopy Good for
Infertility with Endometriosis?
For Stage I and
II endometriosis, surgical excision via laparoscopy roughly doubles monthly
fecundity rates compared with expectant management. This is per Marcoux et al.,
NEJM, 1997 (the Endocan trial) and ASRM Practice Committee 2014. For Stage
III/IV endometriosis, laparoscopy is indicated to restore anatomy. IVF is
typically recommended alongside or immediately after surgery — not waiting for
natural conception. Age matters here. For women over 37 with Stage III/IV
endometriosis, most fertility specialists recommend starting IVF within 3–6
months of surgery.
Laparoscopy & Tubal
Recanalization Cost: India vs Australia, UK & Nigeria (2026)
The
table below covers all key procedures with NGN pricing for Nigerian patients.
This includes pan-endoscopy and both types of tubal recanalization.
|
Procedure |
India
(INR) |
Australia
(AUD) |
Nigeria
(NGN) |
UK
(GBP) |
|
Laparoscopy
for infertility (diagnostic + operative) |
₹70,000–₹1,80,000
($850–$2,200; £680–£1,750) |
AUD
6,000–10,000 |
NGN
500,000–1,500,000 |
£3,000–£6,000 |
|
Laparoscopy
+ Hysteroscopy (combined pan-endoscopy) |
₹1,00,000–₹2,50,000
($1,200–$3,000; £955–£2,390) |
AUD
8,000–14,000 |
NGN
700,000–2,000,000 |
£4,500–£8,000 |
|
Selective
salpingography + tubal cannulation (radiological recanalization) |
₹30,000–₹60,000
($360–$720; £290–£570) |
AUD
3,000–6,000 |
NGN
250,000–600,000 |
£2,000–£4,000 |
|
Microsurgical
tubal reversal (surgical recanalization) |
₹1,50,000–₹3,50,000
($1,800–$4,200; £1,430–£3,330) |
AUD
8,000–15,000 |
NGN
800,000–2,500,000 |
£4,000–£9,000 |
|
Hysteroscopy
alone (diagnostic + operative) |
₹40,000–₹1,20,000
($480–$1,450; £385–£1,155) |
AUD
4,000–8,000 |
NGN
350,000–1,000,000 |
£2,500–£5,000 |
Sources:
These estimates are based on
pricing from leading private hospitals in India, including Apollo Chennai,
Fortis Noida, Medanta Gurugram, and Max Hospitals. In Australia, they reflect
typical private surgical costs for 2025, while in the UK they are aligned with
NHS reference costs (2024–25) and private provider rates such as BMI
Healthcare. For Nigeria, the figures are based on private hospital pricing in
Lagos for 2025. All costs are approximate and can vary depending on
the hospital, anaesthesia, and how simple or complex the procedure is.
For
Nigerian patients, the cost comparison is particularly relevant. Advanced
gynaecological laparoscopy for infertility — with simultaneous operative
treatment — is available at very few centres in Lagos or Abuja. None match the
volume and specialist experience of India’s top fertility hospitals. Divinheal
coordinates direct appointments at partner hospitals in Delhi and Chennai for
Nigerian patients. Flight times from Lagos are approximately 8–10 hours, with
one stop via Dubai or Addis Ababa.
In Australia, you can get an endometriosis
laparoscopy through the public system, but waiting times are often long—around
3 to 12+ months depending on where you are and how urgent the case is. If you
go private, it usually costs about AUD 6,000–10,000. In India, the same surgery
typically costs around ₹70,000–₹1,80,000 (about AUD 1,300–3,300), which is
roughly 60–75% lower than private Australian prices. This comparison is just
for the procedure itself and doesn’t include travel or accommodation costs.
Recovery After Laparoscopy
for Infertility: What to Expect
Recovery Time for Laparoscopy for
Infertility
A standard
laparoscopy for infertility involves a day of surgery or one overnight stay.
This includes operative treatment of mild-to-moderate endometriosis or pelvic
adhesions. Most patients return to light desk work within 3–5 days. Full
recovery, including resumption of exercise and physically demanding work, takes
2–4 weeks. More extensive operative work means longer recovery. Complex
endometriosis excision or myomectomy may need 4–6 weeks.
Immediate
post-operative symptoms include shoulder tip pain from residual CO2 gas — this
resolves within 24–48 hours with gentle walking. Mild abdominal bloating,
fatigue, and small incision site discomfort are also common. These are managed
with prescribed oral pain relief. Most international patients are cleared to
fly home 5–7 days after a standard laparoscopy. Divinheal arranges a minimum
7-night stay near the partner hospital before return travel.
Can You Get Pregnant 1 Month
After Laparoscopy?
In theory, yes —
conception can occur in the first post-operative cycle. In practice, most
fertility specialists advise one full menstrual cycle (4–6 weeks) of healing
before actively trying to conceive. This allows incision sites to heal fully.
It also lets any uterine lining disruption from associated hysteroscopy
resolve. Progesterone supplementation (if prescribed) completes its course, and
the treated pelvic environment stabilises. For extensive operative work —
endometrioma removal, adhesiolysis, or tubal repair — 2–3 months of healing may
be needed. Your surgeon will advise based on what was done. Your surgeon will
advise specifically based on what was done.
When to Try to Conceive After
Laparoscopy
For women with
endometriosis, the post-operative fertility window is 6–12 months. After this,
endometriosis recurrence begins to erode the benefit. Acting within this window
is important — particularly for women over 35 or with reduced ovarian reserve.
For women who had a laparoscopy for unexplained infertility or tubal adhesions
without endometriosis: try to conceive from cycle 2 onward. Discuss IVF at 6
months if no pregnancy has occurred. For women who had tubal recanalization,
try from the first post-procedure cycle. Monitor any early pregnancy with an ultrasound
at 6–7 weeks.
Patient Journeys: Australia,
UK & Nigeria
Sarah, 34 — London, UK
Sarah had five years of unexplained
infertility with normal semen analysis and a clear HSG. Her NHS gynaecologist
listed her for diagnostic laparoscopy — the wait was 14 months. After
consulting Divinheal, she was seen at Fortis Noida within 8 days. Laparoscopy
identified Stage II endometriosis, not visible on her prior MRI. Excision was
completed in the same session. Sarah conceived naturally 7 months
post-procedure. Her total India trip was 9 days. Total cost, including flights
and accommodation, was approximately £2,800. Her UK private surgical quote had
been £5,500 for diagnostic laparoscopy alone — with no operative treatment
included.
The story is an illustrative composite
based on typical patient journeys. Name changed for privacy.
Amara, 31 — Lagos, Nigeria
Amara had been told by her Lagos
gynaecologist that laparoscopy for infertility was not available at sufficient
specialist volume locally. Her diagnosis was possible pelvic adhesions from a
prior infection, with an inconclusive HSG. Divinheal matched her to Apollo
Hospitals Chennai. The laparoscopy confirmed bilateral peritubal adhesions,
which were completely cleared in the same session. Her total procedure and stay
cost NGN 820,000 — including the 3-night post-operative stay. She returned to
Lagos on day 7 with a full operative report in English for her local
gynaecologist.
The story is an illustrative
composite based on typical patient journeys. Name changed for privacy.
James and Natalie — Melbourne,
Australia
Natalie, 36, was on
a 9-month public waiting list for a laparoscopy after a failed IVF cycle, which
raised questions about endometriosis. Divinheal coordinated a combined
laparoscopy-hysteroscopy at Medanta Gurgaon. Laparoscopy found and excised a
Stage III endometrioma; hysteroscopy cleared a small intrauterine adhesion.
Both were done in one 2.5-hour session. They returned to Melbourne 8 days
post-procedure. Total India cost: AUD 4,100. Their Australian private quote for
the laparoscopy alone (without hysteroscopy) had been AUD 9,200.
The story is an
illustrative composite based on typical patient journeys. Names changed for
privacy.
How Divinheal Supports
Patients from Australia, UK & Nigeria
Divinheal matches each patient to the
most suitable NABH-accredited hospital based on their diagnosis, procedure
needs, and budget. For example, Nigerian patients needing advanced laparoscopy
are often referred to Apollo Hospitals Chennai, where appointments are usually
available within 1–2 weeks. UK patients with complex endometriosis may be
guided to Medanta Gurugram for its expertise in high-volume excision surgery, for
Australian patients requiring both laparoscopy and hysteroscopy, Fortis Noida
and Max Hospitals are often preferred, as both procedures can
often be done in one session with international patient support.
What Divinheal Coordinates
•
Clinic matching based on diagnosis, procedure
type, and budget
•
Hospital appointment booking within 1–2 weeks
•
Medical visa invitation letter from the partner
hospital
•
Accommodation 1–2 km from the treatment centre
•
Pickup
and drop services between the airport and hospital/hotel
•
A
dedicated patient coordinator reachable on WhatsApp during the entire stay
•
A
complete operative summary in English for your treating doctor back home
•
Online
follow-up consultations with the specialist after you return
• Divinheal does not charge a placement fee. A written cost estimate in AUD, GBP, or NGN is available before you commit to travel.
Final Thoughts
Laparoscopy
for infertility in India costs ₹70,000–₹1,80,000 at NABH-accredited partner
hospitals — Apollo Chennai, Fortis Noida, and Medanta Gurgaon. That is
$850–$2,200 (£680–£1,750; NGN 500,000–1,500,000; AUD 1,300–3,300). It is 60–75%
less than comparable private gynaecological surgery in Australia or the UK.
For Nigerian
patients, India provides access to specialist laparoscopy with simultaneous
operative treatment that may not be available locally. For Australian and UK
patients, Divinheal eliminates waiting lists that run 6–14 months for NHS
gynaecology. For all three patient groups, a combined laparoscopy-hysteroscopy
pan-endoscopy in India typically costs less than a diagnostic-only laparoscopy
at home.
Reach out to Divinheal for a free case
evaluation. You’ll get help choosing the right procedure, a transparent cost
estimate in your local currency, and a consultation with an experienced
gynaecological surgeon.
Disclaimer: All
cost figures are approximate 2025–2026 estimates for private healthcare.
Individual costs depend on procedure complexity, hospital tier, and patient
protocol. Medical decisions should be made in consultation with a qualified
specialist. Clinical data references: Arab W et al., JBRA Assisted Reproduction
2022 (PMC8769170); Marcoux et al., NEJM 1997; ASRM Practice Committee 2014;
Zondervan et al., Nature Reviews Disease Primers 2018. Patient stories are
illustrative composites; names changed for privacy. All citations should be verified
by the Divinheal medical team before publication.
Related Links
International Patient Visiting India
- ivf in bengaluru for ethiopia
- ivf in pune for bangladesh
- ivf in india for bangladesh
- ivf in mumbai for bangladesh
- ivf in bengaluru for bangladesh
- ivf in pune for uae
- ivf in bengaluru for uae
- ivf in new delhi for uae
- ivf in hyderabad for uae
- ivf in chennai for bangladesh
- ivf in new delhi for iraq
- ivf in bengaluru for iraq
- ivf in mumbai for iraq
- ivf in chennai for iraq
- ivf in bengaluru for nigeria
- ivf in pune for nigeria
- ivf in hyderabad for nigeria
- ivf in india for nigeria
- ivf in india for ethiopia
- ivf in new delhi for ethiopia
Booking With DIVINHEAL
Get a free consultation to understand your treatment options
Related Links
International Patient Visiting India
- ivf in bengaluru for ethiopia
- ivf in pune for bangladesh
- ivf in india for bangladesh
- ivf in mumbai for bangladesh
- ivf in bengaluru for bangladesh
- ivf in pune for uae
- ivf in bengaluru for uae
- ivf in new delhi for uae
- ivf in hyderabad for uae
- ivf in chennai for bangladesh
- ivf in new delhi for iraq
- ivf in bengaluru for iraq
- ivf in mumbai for iraq
- ivf in chennai for iraq
- ivf in bengaluru for nigeria
- ivf in pune for nigeria
- ivf in hyderabad for nigeria
- ivf in india for nigeria
- ivf in india for ethiopia
- ivf in new delhi for ethiopia
DivinHeal's Journey

Latest Articles
Frequently Asked Questions
Get answers to common questions about medical tourism, treatment procedures, and our comprehensive healthcare services.
Ready To Start Your Healing Journey?
Get Personalized Medical Treatment Options From India's Top Hospitals. Our Medical Experts Are Ready To Assist You Every Step Of The Way.