

Written by DivinHeal Editorial Contributor, Samrat Nilesh, Embryologist | Medically Reviewed by Dr Indu Priya, Gynecologist(MBBS,MD) Published on: 2026-05-30
Can Asherman’s Syndrome Cause Weight Gain? Symptoms, Treatment & Pregnancy Outcomes in India
About 1 in 5 women develops Asherman’s syndrome after a uterine procedure. A D&C (dilation and curettage) is the most common trigger. Asherman’s syndrome is a condition where scar tissue forms inside the uterus. This blocks the uterine cavity and disrupts periods and fertility. For many women, the first question after diagnosis is: Can Asherman’s syndrome cause weight gain?
The short answer is no. Asherman’s syndrome does not directly cause weight gain. But knowing why weight changes can happen alongside this condition — and what good treatment looks like — matters a great deal for your recovery and your family plans.
This guide explains what Asherman’s syndrome is and how it is diagnosed. It covers how hysteroscopic adhesiolysis (the surgical removal of uterine scar tissue) is performed at leading hospitals in India. It also shows what fertility outcomes look like after treatment. And it explains how patients from Australia, the UK, and Nigeria get high-quality care at 70–90% less than private clinic prices at home.
What Is Asherman’s Syndrome? (Also Called Asherman Disease)
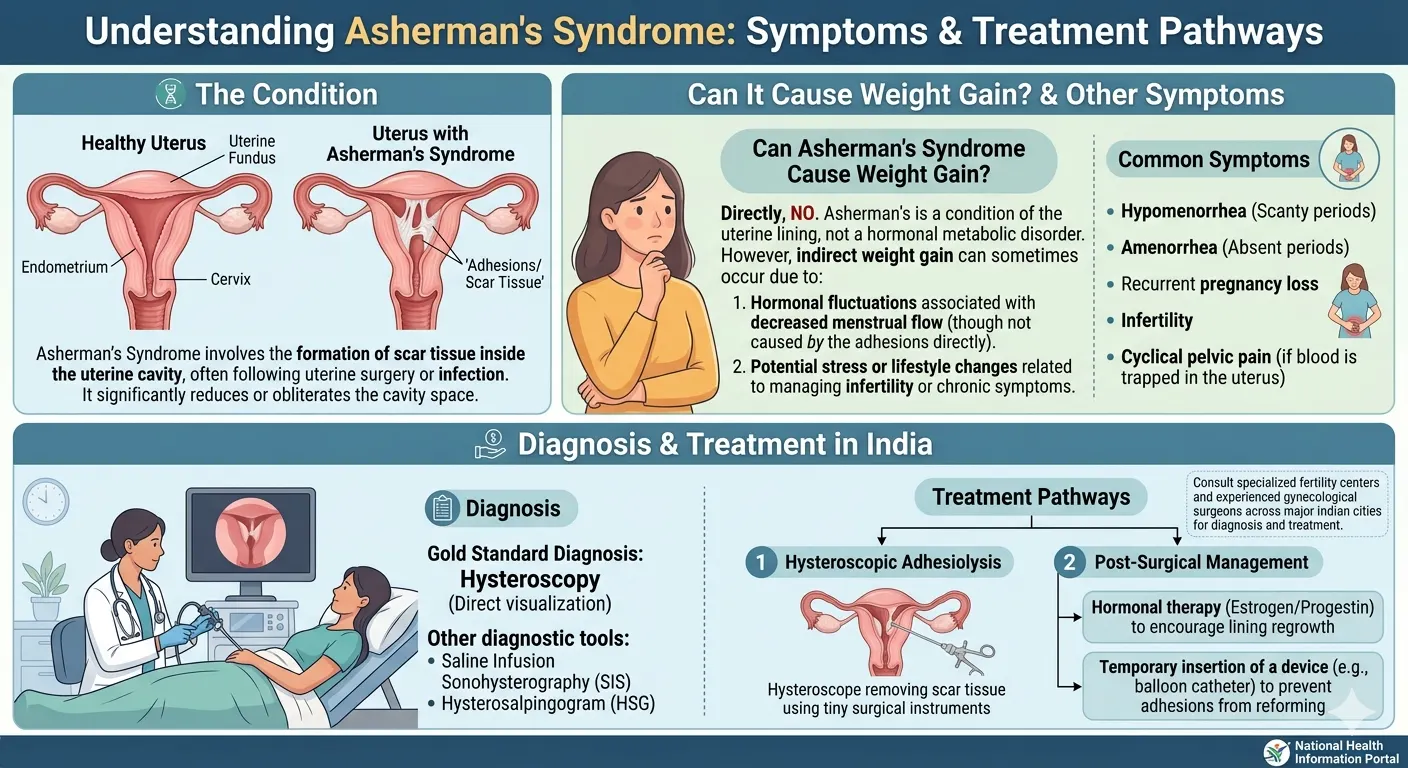
Asherman’s syndrome — also called Asherman disease or intrauterine adhesions — is a condition where scar tissue (adhesions) forms inside the uterine cavity. This scar tissue can partly or fully block the cavity. Dr. Joseph Asherman, an Israeli gynaecologist, first described it in 1948. It remains one of the leading causes of secondary infertility and menstrual problems in women of reproductive age worldwide.
What Causes Asherman’s Syndrome?
Over 95% of Asherman’s syndrome cases are linked to trauma to the uterine lining (endometrium). This trauma almost always comes from surgical procedures on a pregnant or recently pregnant uterus (WHRIA, 2024). The most common trigger is a D&C — especially after a miscarriage, incomplete abortion, or retained placental fragments after delivery.
Studies show Asherman’s syndrome develops in 2–48% of women after surgical removal of an early pregnancy loss. The risk rises sharply when multiple procedures are done or when sharp curettage is used (Journal of Obstetrics and Gynaecology Canada, 2016).
Other causes include:
Myomectomy (surgical removal of uterine fibroids)
C-section complications or uterine repair surgery
Severe uterine infections such as endometritis
Radiation therapy directed at the pelvis
The Classic Triad of Asherman Syndrome Symptoms
Asherman syndrome is known by three connected symptoms. Doctors call this the Asherman triad:
Amenorrhoea or hypomenorrhoea — absent or dramatically reduced menstrual flow, even though your hormone levels are normal. This happens because the scar tissue blocks menstrual blood from exiting the uterus.
Cyclical pelvic pain — you may still feel the cramping of a menstrual cycle, but blood builds up behind the adhesions and cannot drain properly. This causes significant discomfort.
Infertility or recurrent miscarriage — the altered uterine environment prevents embryo implantation or disrupts early pregnancy development. This is often how Asherman’s is first identified in women who had no known uterine procedure risk.
If you notice a sudden drop in period flow after a D&C, miscarriage management, or any uterine surgery, tell your gynaecologist right away. Early diagnosis leads to better treatment outcomes.
Does Asherman’s Syndrome Cause Weight Gain?
No. Asherman’s syndrome does not directly cause weight gain. The adhesions (scar tissue) form inside the uterine cavity. They have no effect on your metabolism, hormones, or fat storage (American Society for Reproductive Medicine).
That said, some women do notice weight changes around the time of diagnosis. These are almost always linked to indirect factors:
Stress and psychological impact — dealing with infertility, recurrent miscarriage, or absent periods takes a real emotional toll. Chronic stress can alter eating patterns and physical activity levels.
Post-surgical recovery — in the weeks after a D&C or hysteroscopy, reduced activity temporarily affects your energy balance.
Co-existing conditions — if your Asherman’s followed a complicated pregnancy or postpartum event, you may also have a thyroid change or other hormonal shift. These are separate from the Asherman’s itself but are worth investigating alongside it.
If you have both menstrual changes and unexplained weight changes, tell your specialist about both. Thyroid function tests and other hormonal markers are worth checking alongside an Asherman’s evaluation.
How Is Asherman’s Syndrome Diagnosed?
Asherman’s syndrome needs a specialist gynaecological assessment to diagnose. A symptom pattern alone is not enough. A definitive diagnosis requires direct visualisation of the uterine cavity.
Hysteroscopy — The Gold Standard Diagnostic Test
Hysteroscopy is a procedure where a thin, lighted camera (hysteroscope) is passed through the cervix into the uterine cavity. It lets the gynaecologist see the adhesions directly — their location, density, and how much of the cavity they affect. It is the only method that confirms the diagnosis with certainty.
The procedure is typically done as a day case under light sedation or local anaesthesia. Leading centres such as Apollo Hospitals Chennai and Fortis Memorial Research Institute, Gurugram, perform over 1,000 hysteroscopic procedures each year — including complex Asherman’s cases referred from Australia, the UK, and Nigeria.
The Royal College of Obstetricians and Gynaecologists (RCOG) recommends hysteroscopy as the definitive investigation when intrauterine adhesions are suspected (RCOG, 2023).
Supporting Diagnostic Tests
Two non-invasive tests are often used when hysteroscopy is not immediately available, or as a first assessment:
Saline Infusion Sonography (SIS) — an ultrasound where saline solution is gently injected into the uterus to outline the cavity. It can identify filling defects and irregular areas where adhesions may be present.
Hysterosalpingogram (HSG) — an X-ray using contrast dye that maps the uterine cavity shape and checks whether the fallopian tubes are open. It can suggest but not confirm Asherman’s.
Neither test replaces hysteroscopy. But both can guide whether urgent specialist referral is needed. This is especially useful for Nigerian patients, where advanced diagnostic tools may not always be locally available.
Hysteroscopic Adhesiolysis — The Gold Standard Treatment for Asherman’s Syndrome in India
Hysteroscopic adhesiolysis is the main and most effective treatment for Asherman’s syndrome. It is minimally invasive and safe when performed by an experienced surgeon. It is highly effective — with success rates of 70–90% for restoring normal uterine anatomy in mild-to-moderate cases (multiple peer-reviewed studies, including ACOG clinical guidance, 2020).
What Happens During Adhesiolysis?
During the procedure, your surgeon inserts a hysteroscope through the cervix into the uterine cavity. The surgeon uses small scissors or a bipolar energy instrument to carefully cut and remove the scar tissue. The goal is to restore the uterine cavity to its normal shape. This allows the endometrium (uterine lining) to grow back and function normally.
The procedure takes 30–60 minutes under general or regional anaesthesia. Most patients go home the same day or after one night in the hospital.
In India, leading JCI-accredited hospitals such as Apollo Hospitals (Chennai and Delhi), Max Healthcare (Delhi), and Fortis Memorial Research Institute (Gurugram) employ gynaecologists with FRCS, MCh, and DNB qualifications. These surgeons perform hundreds of adhesiolysis procedures each year. They follow protocols that match private gynaecology centres in Sydney or London — at a fraction of the cost.
Post-Operative Care and Preventing Recurrence
Post-operative care is just as important as the surgery itself. After your adhesiolysis, your medical team in India will typically:
Insert a small intrauterine balloon for 5–7 days to keep the uterine walls separated while healing begins
Prescribe a course of oestrogen therapy — sometimes combined with progestins — to encourage healthy endometrial regrowth and reduce the chance of new adhesions forming
Apply an anti-adhesion gel or barrier directly inside the uterus during surgery as an extra layer of protection
Schedule a follow-up hysteroscopy 4–6 weeks after your procedure to check for any new adhesion formation
Post-operative hormonal therapy has been shown to reduce Asherman’s recurrence rates from an average of 15–20% down to below 5–10% for mild-to-moderate cases (WHO, 2021). With the right post-op care, most patients do not need a second procedure.
Can You Get Pregnant After Asherman’s Syndrome? What to Expect
Yes, many women can become pregnant after treatment for Asherman’s syndrome. Live birth rates following successful adhesiolysis are 70-80% in those with mild-to-moderate adhesions (ACOG, 2020). Rates are lower in severe cases but can be further optimised with IVF after adhesiolysis.
Fertility Outcomes After Adhesiolysis
Your fertility outcomes depend on three key factors:
Severity of adhesions before treatment — mild and moderate cases respond best to a single adhesiolysis procedure. Severe cases may require two or three procedures over 12–18 months.
Surgeon experience — specialists performing 200+ hysteroscopies annually consistently achieve better cavity restoration and lower recurrence rates.
Post-operative compliance — completing the full hormonal therapy course and attending all follow-up appointments is critical for sustained success.
Amaka, a 33-year-old woman living in Lagos, was found to be suffering from moderate Asherman’s syndrome due to two D&Cs carried out post a miscarriage. She was able to conceive naturally nine months after undergoing hysteroscopic adhesiolysis surgery in an accredited Delhi hospital through Divinheal. “They were very meticulous about the whole process, and I felt really well taken care of. It cost less than one appointment would have done in a London private hospital,” Amaka added.Illustrative composite based on typical patient journeys. Name changed for privacy.
Pregnancy Risks to Monitor After Asherman’s Syndrome
Even after successful treatment, pregnancies after Asherman’s syndrome carry an elevated risk profile that needs close obstetric monitoring. These risks include:
Higher likelihood of first-trimester miscarriage
Preterm labour and delivery
Abnormal placental implantation — placenta previa (placenta positioned over the cervix) or placenta accreta (placenta growing into the uterine wall)
Postpartum haemorrhage (heavy bleeding after delivery)
Your medical team in India will advise a waiting period of 6–12 months after adhesiolysis before trying to conceive. This gives the uterine lining time to stabilise. Once pregnant, close monitoring from early in the first trimester is essential. Your Indian hospital will provide a full discharge summary and follow-up plan for your obstetrician at home.
Asherman’s Syndrome Treatment Cost: India vs Australia, Nigeria & the UK
Treating Asherman’s syndrome in India costs between ₹1,50,000 and ₹3,50,000 (approximately USD 1,800–4,200). At leading JCI-accredited hospitals, this typically includes the surgeon’s fee, anaesthesia, a 2–3 night hospital stay, pre-operative investigations, and post-operative consultations. Some packages also include airport transfer and accommodation coordination.
Country | Estimated Cost (Local Currency) | Approx. USD | Savings vs India | Key Context |
India | ₹1,50,000 – ₹3,50,000 | $1,800 – $4,200 | — | JCI-accredited hospitals, FRCS surgeons |
Australia | AUD 15,000 – AUD 25,000 | $10,000 – $16,500 | 75–90% | Medicare wait-list: 6–12 months for non-urgent cases |
United Kingdom | £8,000 – £15,000 | $10,000 – $19,000 | 70–85% | NHS wait-list: 3–6 months; private = significant cost |
Nigeria | NGN 3,000,000 – 7,500,000 | $2,000 – $5,000 | 40–60% + advanced tech access | Limited advanced hysteroscopic equipment locally |
All figures are indicative only. Cost may vary depending upon the class of hospital, seniority of the surgeon, and difficulty level of the surgery.
Divinheal will provide you with an individual quote.
Why Australian and UK Patients Choose India
Australian Medicare waiting time for non-emergency gynaecological surgery is 6-12 months (Medicare statistics, 2023). Private adhesiolysis treatment in Sydney or Melbourne will cost AUD 15,000-25,000 — an expensive procedure even on a private health insurance plan. An Indian option helps Australian patients save 75-90% of costs and get treated within 2-4 weeks of inquiry.
UK patients face NHS wait-lists of 3–6 months for elective hysteroscopy. Private NHS-equivalent care starts at £8,000. Indian hospitals offer the same surgical standards — many surgeons hold FRCS qualifications — at 70–85% less.
Why Nigerian Patients Choose India
For patients in Lagos, Abuja, or Port Harcourt, the challenge is often access as much as cost. Advanced operative hysteroscopy — needed for moderate-to-severe Asherman’s — is not always available at private facilities locally. India provides that access, along with Divinheal’s step-by-step visa application support, flight coordination, and on-ground assistance from arrival to discharge.
Is Medical Travel to India for Asherman’s Syndrome Safe?
Yes — medical travel to India for Asherman’s syndrome treatment is safe. You need to choose an internationally accredited hospital and an experienced gynaecologist. India has over 40 JCI (Joint Commission International)-accredited hospitals. JCI accreditation is the global benchmark for hospital quality and patient safety. It means the facility meets strict international standards across surgical protocols, infection control, and patient care.
What Accreditation Means for You
Indian JCI hospitals are audited externally. For patients originating from Australia and the United Kingdom, this provides the same reassurance that they would receive when choosing a private hospital in their own country. The number of hysteroscopy cases performed each year by Apollo Hospitals Chennai exceeds 2,000, thereby developing their surgical and management skills in handling potential complications. NABH (National Accreditation Board for Hospitals) accreditation provides a parallel domestic quality benchmark.
Indian gynaecologists at these centres often hold postgraduate qualifications from UK or Australian training programmes — FRCS, MRCOG, or DNB. They know the clinical expectations of international patients.
How to Evaluate Hospitals and Reviews
While conducting an online search for hospitals, always try to find reviews that include specific treatments, surgeon names, and actual patients' experiences, rather than the number of stars given to them. It would be important to observe consistencies across several sources, including Google Reviews, health tourism forums, and patient reviews. Pay attention to how hospitals respond to critical feedback. Transparency is a genuine quality signal.
Divinheal pre-vets all partner hospitals before recommending them. Each hospital on the Divinheal network has been assessed for accreditation status, hysteroscopy volume, surgeon credentials, and international patient support.
How Divinheal Supports You Before, During, and After Treatment
Travelling abroad for gynaecological surgery can feel daunting — especially for patients managing this alone, away from their usual support system. Divinheal provides end-to-end coordination so you can focus on your health, not logistics.
Before You Travel
Divinheal assists with visa applications — a top priority for Nigerian patients applying for an Indian medical visa. The team arranges virtual consultations with FRCS or MRCOG-qualified surgeons, so you can ask questions and review your case before booking flights. Flight and accommodation near your treating hospital are coordinated in advance.
Sarah, who lives in Perth, had to go through hysteroscopic adhesiolysis after a few D&Cs following a miscarriage. She felt nervous about travelling alone. “Divinheal set me up with a patient manager before I even booked my flights,” she said. By the time she arrived in Chennai, she already knew her surgeon, her hospital, and what the whole process would look like.Composite for representation. Name changed for privacy.
During Your Stay
Once you arrive, Divinheal's ground staff will take care of the airport transfer and hospital admission for you. You will have your own patient manager on standby during your stay. Should you require a multilingual interpreter, this can be prearranged for you. Packages for treatment of Asherman's adhesiolysis usually consist of 2-3 days' post operative stay at the hospital, giving you time to recover before moving to your accommodation.
After You Return Home
Divinheal arranges follow-up consultations remotely with your treating physician, normally within two weeks, one month, and three months after the procedure. The GP in Sydney, London, Lagos, or Abuja gets a comprehensive discharge report on your diagnosis, surgery results, medication regimen, and follow-up procedure
Divinheal’s team responds to patient queries within one hour, including after you’ve returned home. Medicare covers local GP visits in Australia, but it does not cover teleconsultations with overseas specialists. Divinheal will clarify any cost implications before you travel.
What Happens After You Return Home? Post-Treatment Care Guide
Managing your recovery after returning home from India needs a clear plan and close communication with both your overseas specialists and your local GP. Here’s what to expect.
Item | What It Covers | Purpose |
Comprehensive Discharge Summary | Diagnosis, surgical findings, medication list, follow-up schedule | For your local GP and ongoing care coordination |
Medication Supply | 1–2 months of prescribed medications (typically oestrogen therapy) | Continuity until your GP issues a local prescription |
Direct Contact Details | Your surgeon’s contact and Divinheal’s 24/7 patient support line | For urgent medical or logistical queries after return |
Local GP Appointment | Schedule within 1–2 weeks of returning home | Handover of overseas treatment to local care |
Teleconsultation Schedule | Divinheal-coordinated follow-up calls with your treating specialist in India | Ongoing specialist oversight without returning to India |
The time frame for recovery from Asherman's syndrome before attempting fertility treatments is 6 to 12 months. Over 75% of all patients respond positively in terms of their treatment outcome when provided with follow-ups (several peer-reviewed journals between 2020 and 2023). You may contact your general practitioner for prescriptions related to hormone therapy and referral to a gynaecologist.
Long-Term Outcomes After Asherman’s Syndrome Treatment
With the right treatment and consistent follow-up, most women achieve a good long-term outcome after Asherman’s syndrome adhesiolysis. The three markers of success are:
Return of a regular menstrual cycle within 2–3 months post-procedure
No recurrence of adhesions on follow-up hysteroscopy at 4–6 weeks
Conception within 12–24 months, for women actively trying to conceive
Recurrence Risk and How to Minimise It
Asherman’s syndrome can come back after treatment, especially in severe cases where dense adhesions cover most of the uterine cavity. Recurrence happens when new scar tissue forms during the post-operative healing phase. Immediate post-operative hormonal therapy — combined with an intrauterine balloon or barrier — significantly lowers this risk: from 15–20% down to below 5–10% in mild-to-moderate cases (WHO, 2021).
If the case is mild, treatment usually bumps pregnancy rates up to 70–80%. Miscarriage rates drop compared to women who don’t get treated for Asherman’s, which isn’t just hearsay—several peer-reviewed studies and NICE guidelines back this up. But if the case is severe, it often takes two or three procedures spread out over a year or so to really get the cavity back to normal.
Factors That Influence Long-Term Fertility
Your long-term fertility outcomes after Asherman’s treatment depend mainly on:
Severity of adhesions before treatment — mild and moderate cases have the best prognosis
Surgeon experience — specialists performing high volumes of hysteroscopy annually achieve consistently better cavity restoration
Adherence to post-operative care — hormone therapy and follow-up hysteroscopy are not optional; they directly determine whether the uterus heals cleanly
Your age and overall reproductive health — younger patients with no other fertility factors typically have the strongest outcomes
India’s leading gynaecology centres offer a level of Asherman’s expertise that matches the best private reproductive surgery units in Sydney, London, or Lagos — at a price that makes treatment accessible rather than out of reach. For many international patients, that difference is life-changing.
Quick Answer — At a Glance
Skim this if you’re short on time.
Asherman’s Syndrome — Key Facts
What it is: Asherman’s syndrome (Asherman disease) is the formation of scar tissue (adhesions) inside the uterus, usually after a D&C procedure, miscarriage management, or uterine surgery
Does it cause weight gain: No — Asherman’s syndrome does not directly cause weight gain. The adhesions affect the uterine cavity only, not metabolism or hormones
Main symptoms: Absent or very light periods (amenorrhoea/hypomenorrhoea), cyclical pelvic pain, and infertility or recurrent miscarriage — the classic Asherman triad
Gold standard treatment: Hysteroscopic adhesiolysis — minimally invasive removal of scar tissue; 70–90% success rate in mild-to-moderate cases
India treatment cost: ₹1,50,000 – ₹3,50,000 (USD 1,800–4,200) at JCI-accredited hospitals
Savings vs home country: 75–90% less than private clinics in Australia; 70–85% less than private clinics in the UK
Pregnancy after treatment: Possible — live birth rates of 70–80% for mild-to-moderate cases after successful adhesiolysis
Who Divinheal connects you with: JCI-accredited hospitals in India with FRCS/MCh-qualified gynaecologists, plus full logistics support from visa to discharge
Related Links
International Patient Visiting India
- ivf in bengaluru for ethiopia
- ivf in pune for bangladesh
- ivf in mumbai for bangladesh
- ivf in bengaluru for bangladesh
- ivf in pune for uae
- ivf in bengaluru for uae
- ivf in new delhi for uae
- ivf in hyderabad for uae
- ivf in chennai for bangladesh
- ivf in new delhi for iraq
- ivf in bengaluru for iraq
- ivf in mumbai for iraq
- ivf in chennai for iraq
- ivf in bengaluru for nigeria
- ivf in pune for nigeria
- ivf in hyderabad for nigeria
- ivf in new delhi for ethiopia
- ivf in hyderabad for bangladesh
- ivf in mumbai for uae
- ivf in pune for iraq
Booking With DIVINHEAL
Get a free consultation to understand your treatment options
Related Links
International Patient Visiting India
- ivf in bengaluru for ethiopia
- ivf in pune for bangladesh
- ivf in mumbai for bangladesh
- ivf in bengaluru for bangladesh
- ivf in pune for uae
- ivf in bengaluru for uae
- ivf in new delhi for uae
- ivf in hyderabad for uae
- ivf in chennai for bangladesh
- ivf in new delhi for iraq
- ivf in bengaluru for iraq
- ivf in mumbai for iraq
- ivf in chennai for iraq
- ivf in bengaluru for nigeria
- ivf in pune for nigeria
- ivf in hyderabad for nigeria
- ivf in new delhi for ethiopia
- ivf in hyderabad for bangladesh
- ivf in mumbai for uae
- ivf in pune for iraq
Meet Our Doctors
Meet our team of highly qualified and experienced medical professionals dedicated to providing the best healthcare services.

Dr Aditi Dixit
Sr. Consultant – Women Imaging
Radiology
New Delhi
15+ Years
Experience
Artemis Hospital
Hospital
1500
Fees

Dr. Alka Gujral
Senior Consultant
Obstetrics and Gynaecology
New Delhi
24+ Years
Experience
Apolo Delhi
Hospital
1500
Fees

Dr. Anita K. Sharma
Senior Consultant - Obstetrics and Gynaecology
Obstetrics and Gynaecology
New Delhi
24+ Years
Experience
Apolo Delhi
Hospital
1500
Fees

Dr. Anjali Bhutani
Senior Consultant
Obstetrics & Gynaecology
New Delhi
22+ Years
Experience
Apolo Delhi
Hospital
1500
Fees

Dr. Aparna Dhar
Senior Consultant - Obstetrics & Gynaecology
Obstetrics & Gynaecology
New Delhi
23+ Years
Experience
Apolo Delhi
Hospital
1500
Fees

Dr. Babita Jain
Principal Director & HOD
Paediatrics (Ped)
New Delhi
30+ Years
Experience
Max Hospital,Gurgaon
Hospital
1500
Fees

Dr Chandrima Misra M
Co-Head Psychological Services
Mental Health and Behavioural Sciences
New Delhi
15+ Years
Experience
Artemis Hospital
Hospital
1500
Fees

Dr. Charu Garg
Principal Director - Radiation Oncology
Radiation Oncology
New Delhi
23+ Years
Experience
Max Hospital,Gurgaon
Hospital
1500
Fees

Dr. Gyanendra Agrawal
Director - Obstetrics & Gynaecology
Obstetrics & Gynaecology
New Delhi
18+ Years
Experience
Apolo Delhi
Hospital
1500
Fees

Dr. Kanika Gupta
Principal Director – Surgical Oncology (Gynae & Robotic Surgery)
Gynecologic Oncology, Robotic & Laparoscopic Surgery, Gynae Cancer Care, Surgical Oncology
New Delhi
39+ Years
Experience
Max Hospital,Gurgaon
Hospital
1500
Fees
DivinHeal's Journey

Latest Articles






Hospitals Offering this treatment
India offers premium medical procedures at affordable prices. Discover our most popular treatments, delivered by the country's finest doctors.

Hisar Intercontinental Hospital
Saray Mah. Siteyolu Cad. No:7, Umraniye, 34768, Istanbul, Turkey
Hisar Intercontinental Hospital

Medical Park Group, Istanbul
Fahrettin Kerim Gokay Cad. Tıbbiye Cd., Kadikoy, Istanbul, Turkey
Medical Park Group, Istanbul

Emsey Hospital, Pendik, Istanbul
Çamlık, Selçuklu Cd. No:22, 34912 Pendik/İstanbul, Türkiye
Emsey Hospital, Pendik, Istanbul


American Hospital, Istanbul
Guzelbahce Sk. No:20, 34365, Nisantasi, Istanbul, Turkey
American Hospital, Istanbul

Memorial Hospitals Group
Burhaniye, Nagehan Sokağı No:4/A D:1, 34676 Üsküdar/İstanbul, Türkiye
Memorial Hospitals Group

Florence Nightingale Hospital Istanbul
Abide-i Hürriyet Cd No:166, 34381 Sisli, Istanbul
Florence Nightingale Hospital Istanbul

Medicana International Hospital, Istanbul
Halit Ziya Turkkani Mah. Medikal Park Cd. No:1, Beylikdüzü, İstanbul
Medicana International Hospital, Istanbul

Okan University Hospital Istanbul
Icmeler Mah. Aydınlıyolu Cd. No:2, 34947 Icmeler-Tuzla, Istanbul
Okan University Hospital Istanbul

Kolan International Hospital, Istanbul
Kaptanpasa Mah. Okmeydan Kavsagi, Darulaceze Cd. No:14, 34384 Sisli, Istanbul
Kolan International Hospital, Istanbul
Frequently Asked Questions
Get answers to common questions about medical tourism, treatment procedures, and our comprehensive healthcare services.
Ready To Start Your Healing Journey?
Get Personalized Medical Treatment Options From India's Top Hospitals. Our Medical Experts Are Ready To Assist You Every Step Of The Way.