

Written by DivinHeal Editorial Contributor, Samrat Nilesh, Embryologist | Medically Reviewed by Dr Indu Priya, Gynecologist(MBBS,MD) Published on: 2026-05-24
Endometriosis: 20 Symptoms, Surgery, Stage 4 and Adenomyosis Differences
Priya, 29, from Sydney, spent three years being told her severe pelvic pain was “just bad periods.” By the time a specialist saw her, she had Stage 3 endometriosis with two ovarian endometriomas. She found Divinheal, flew to Apollo Hospitals in Chennai, and had laparoscopic excision by an FRCS-trained endometriosis surgeon within two weeks of her first inquiry. Total cost: INR 2,10,000 — 62% less than the AUD 11,000 she had been quoted privately in Sydney. She returned home 10 days after surgery with a written post-operative care plan for her GP.
This guide covers everything. You’ll find the 20 symptoms of endometriosis and how the four stages work. You’ll learn what makes Stage 4 different, how it compares to adenomyosis, and whether it can cause cancer. Surgery, recovery, and treatment costs in India versus the UAE, UK, and Australia are all covered.
What Is Endometriosis and Who Does It Affect?
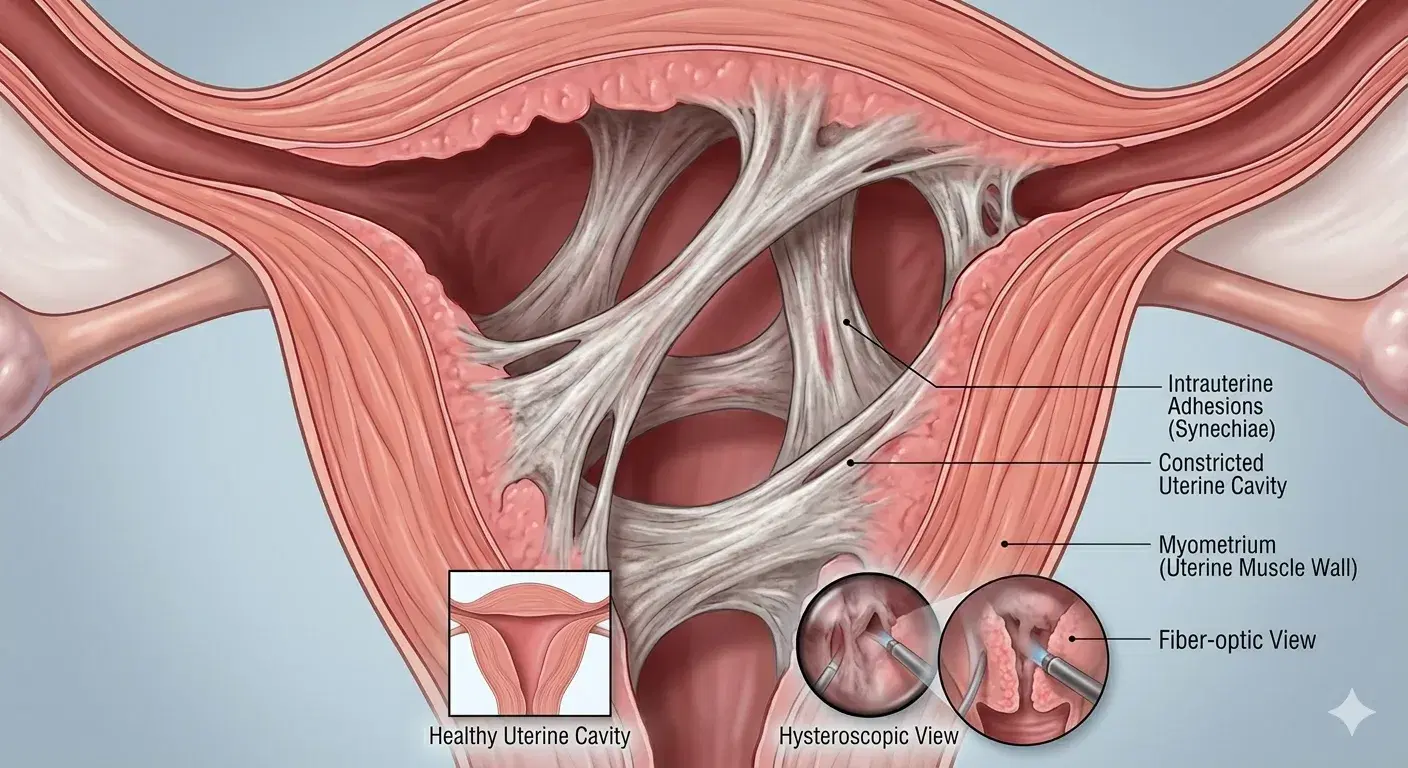
Endometriosis is a condition where tissue like the uterine lining grows outside the uterus. It can grow on the ovaries, fallopian tubes, bowel, bladder, and in severe cases the diaphragm or abdominal wall. Each month, hormones cause this tissue to build up and bleed — just as the uterine lining does. But this blood has nowhere to go. Over time, this causes inflammation and scarring. The body forms adhesions — tough bands of scar tissue that bind organs together. This leads to significant pain and, in many cases, fertility problems.
Endometriosis occurs in about one in ten women of reproductive age around the globe, affecting an estimated 190 million women across the world (WHO, 2023). This disease tends to occur mostly among women aged 25 to 40 years, although the onset of symptoms may start much earlier in the teenage years. On average, there is a delay of six to nine years from the onset of symptoms to diagnosis in the UK and Australia (NICE, 2022; Endometriosis Australia, 2023). This delay happens because symptoms are often dismissed. NHS gynaecology referral wait times average 12+ months.
What Are the Red Flag Symptoms of Endometriosis?
Not all pelvic pain is endometriosis. But if you have these red flag symptoms, see a specialist. Don’t keep waiting:
Period pain so severe that it stops you from going to work, school, or social activities
Pelvic pain that persists outside your period — present on days you are not bleeding
Deep pain during or after sexual intercourse that does not resolve
Painful bowel movements or urination, especially during your period
Unexplained difficulty conceiving or recurrent miscarriage
Fatigue is so severe that it interferes with normal daily function during your period
Persistent lower abdominal bloating (“endo belly”) unrelated to food intake
The presence of three or more symptoms is an indication for a specialist referral, which takes on average between 6-18 months through the NHS or Australian Medicare routes. Consultations are made by Divinheal to JIC-accredited hospitals in India within 5-10 working days.
The 20 Symptoms of Endometriosis You Should Know
Endometriosis is often misdiagnosed as irritable bowel syndrome, pelvic inflammatory disease, or simply heavy periods. Knowing the full range of symptoms helps you push for a proper diagnosis. Below are 20 documented symptoms, grouped by type.
The 4 D’s of Endometriosis: Dysmenorrhea, Dyspareunia, Dyschezia, Dysuria
Doctors use the “4 D’s” as a diagnostic guide. These four symptoms are the most consistent and important signs of endometriosis (PMC, ENDOPAIN-4D study, 2021):
Dysmenorrhea (severe period pain): Not ordinary cramping — pain that is much worse than normal, often starting 1-2 days before bleeding, lasting throughout the period. Women frequently describe it as deeper and more constant than labour contractions. It typically worsens with each cycle without treatment.
Dyspareunia (painful intercourse): Deep pain during or after sex, particularly with deep penetration. Affects approximately 60% of women with deep infiltrating endometriosis (NHS). It can severely impact intimate relationships and mental health over time.
Dyschezia (painful bowel movements): Pain when opening the bowels, especially during your period. Endometrial lesions on or near the bowel cause straining, urgency, and sometimes rectal bleeding during menstruation.
Dysuria (painful urination): Burning sensation, frequency, or urgency when urinating. When endometriosis affects the bladder, it mimics a urinary tract infection — but urine cultures are clear. This is bladder endometriosis.
The Full 20 Symptoms: Beyond the 4 D’s
Beyond the 4 D’s, endometriosis causes many other symptoms throughout the body. Doctors often dismiss these or blame other conditions:
Severe, progressively worsening period pain (dysmenorrhea)
Chronic pelvic pain — persisting throughout the month, not only during periods
Deep pain during or after sex (dyspareunia)
Painful bowel movements, particularly cyclically (dyschezia)
Painful urination during menstruation (dysuria)
Heavy or prolonged menstrual bleeding
Spotting or bleeding between periods
Abdominal bloating (“endo belly”) — sudden, unrelated to food, often worse during period
Nausea and vomiting during menstruation
Debilitating fatigue — particularly in the week before and during your period
Low back pain, often radiating or described as deep and constant
Leg or sciatic-type pain — when lesions affect pelvic nerves
Shoulder tip pain — when diaphragmatic lesions irritate the phrenic nerve
Constipation, diarrhoea, or alternating bowel habits — cyclically worse around periods
Rectal bleeding during menstruation
Difficulty conceiving or unexplained infertility — affects 30-50% of women with endometriosis (WHO, 2023)
Recurrent miscarriage
Cyclical chest pain or breathlessness — rare, indicates thoracic endometriosis
Depression, anxiety, and emotional distress — linked to chronic pain and diagnostic delay
Reduced quality of life affecting work, relationships, and social engagement
What Organs Can Endometriosis Affect?
Endometriosis most commonly affects:
Ovaries — forming endometriomas (“chocolate cysts”) filled with old blood
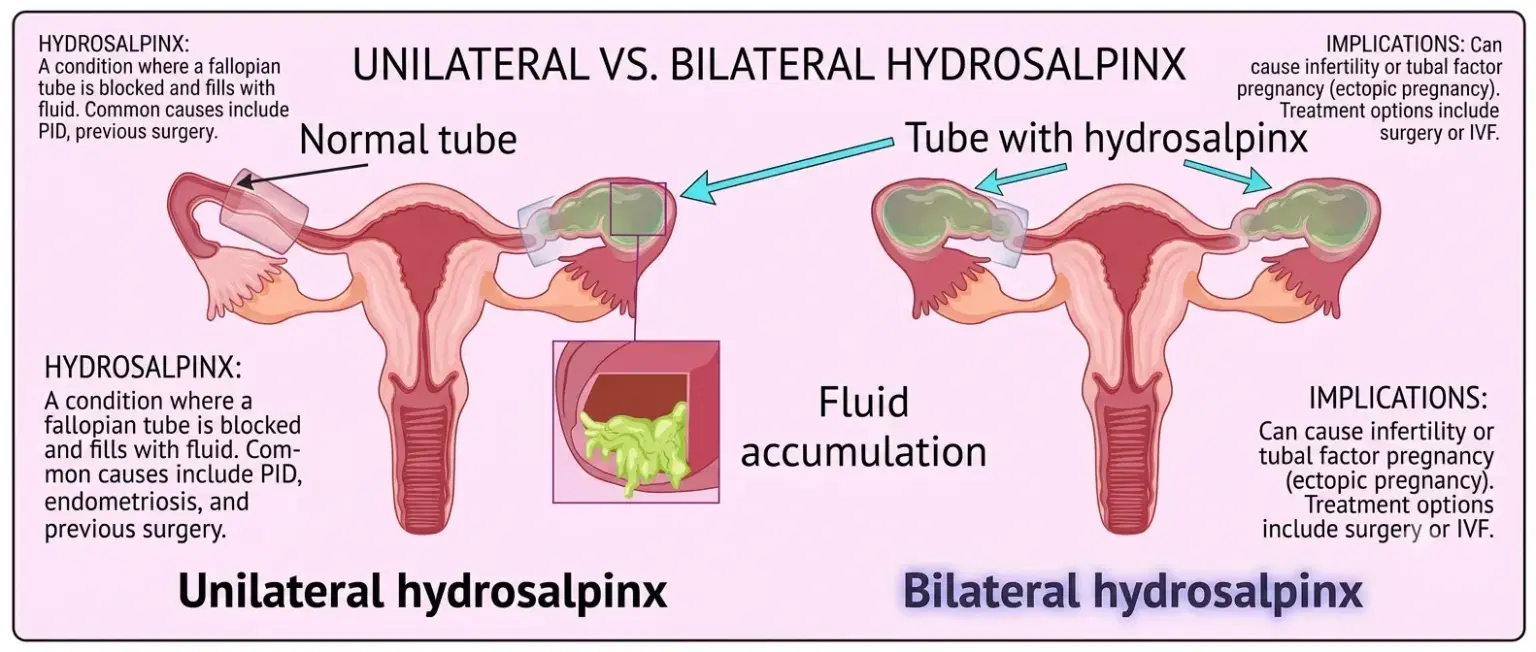
Fallopian tubes — causing blockage and reducing fertility
The peritoneum — the lining of the pelvic and abdominal cavity
Bowel and rectum — causing bowel endometriosis with dyschezia and rectal bleeding
Bladder and ureters — causing bladder endometriosis with dysuria
The rectovaginal septum — a common site for deep infiltrating endometriosis
In rare cases, endometriosis is found on the diaphragm, causing cyclical chest pain. It can also appear inside the lungs (catamenial pneumothorax) or in caesarean section scars. Where the lesions grow determines which symptoms you get. This is why endometriosis looks so different from woman to woman.
Endometriosis Stages: What Stage 1 Through Stage 4 Actually Mean
Endometriosis is classified into four stages by the revised American Society for Reproductive Medicine (rASRM) scoring system. The score is based on the number, size, and depth of implants, the presence of ovarian cysts, and the degree of adhesions. Here’s a key fact: stage does not reliably predict how much pain you feel. A woman with Stage 1 can have severe pain. A woman with Stage 4 may feel less pain but struggle with infertility. The stage describes how widespread the disease is, not how much you suffer.
Stages 1 to 3: Minimal, Mild, and Moderate Endometriosis
Stage | Classification | What You Will Find | Key Features |
Stage 1 | Minimal | Few shallow implants | Isolated lesions, no adhesions, no cysts |
Stage 2 | Mild | More and deeper implants | Scarring beginning; no significant adhesions |
Stage 3 | Moderate | Many deep implants; cysts on at least one ovary | Adhesions affecting tubes or ovaries; the fertility impact begins |
What are the symptoms of Stage 3 endometriosis? Stage 3 usually causes pelvic pain that doesn’t stop on period days — it carries on. Intercourse becomes more painful with each cycle. Fertility problems start to show. Ovarian endometriomas cause a dull, steady ache that doesn’t go away between periods. Many women at Stage 3 say their symptoms have built up over the years to the point of affecting their ability to work.
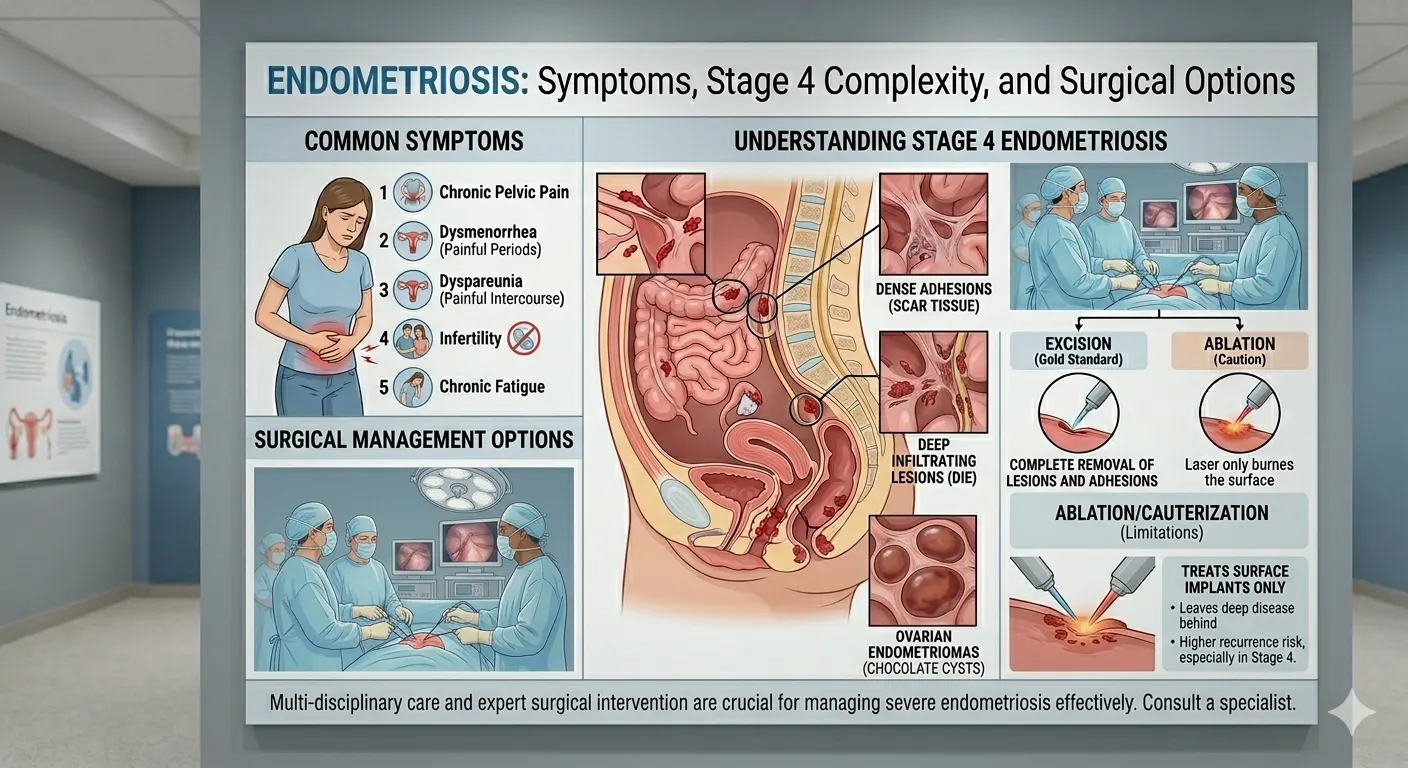
Stage 4 Endometriosis: How Serious Is It and What Does It Feel Like?
Stage 4 endometriosis is the most severe classification, with:
Many deep endometrial implants throughout the pelvis
Large endometriomas on one or both ovaries — often 4cm or larger
Thick, dense adhesions that bind organs together: ovaries to uterus, bowel to uterus, bladder to uterus, or bowel to bladder
Significant distortion of normal pelvic anatomy (Centre of Endometriosis, 2022)
How serious is Stage 4 endometriosis? Stage 4 carries the highest risk of infertility. Natural conception rates are much lower than in unaffected women. Dense adhesions can block the bowel or bladder in the most severe cases. Surgery is complex and requires a team of specialists working together.
What does Stage 4 endometriosis feel like? Women with Stage 4 describe pain that is no longer only during their period. It is there every day, often spreading into the back and legs. Sex may become impossible. Everyday tasks — sitting for long, using the bathroom, even walking — can trigger pain. Depression and anxiety are more common at Stage 4 than in the general population (PMC, 2021).
What is the life expectancy of someone with Stage 4 endometriosis? The condition of endometriosis does not affect the life expectancy of any individual. This condition is non-malignant. The minor increase in the risk of some ovarian cancers does not have a huge effect on the life span of patients. Quality of life becomes an important aspect. Regular gynaecological review every 1-2 years is recommended for monitoring.
Can you heal Stage 4 endometriosis? There is no cure, but Stage 4 can be effectively managed. Laparoscopic excision surgery removes all visible lesions and adhesions. It produces significant and lasting pain relief in most patients. The surgeon must be skilled in deep infiltrating endometriosis. Post-surgical hormonal therapy reduces recurrence rates. At Divinheal’s partner hospitals in India, Stage 4 excision is performed by teams including gynaecological surgeons, colorectal surgeons, and urologists. This team approach is essential when the bowel or bladder is involved.
Deep Infiltrating Endometriosis: Why It Is Different and Harder to Treat
Deep infiltrating endometriosis (DIE) occurs when lesions grow more than 5mm deep into an organ. This can happen in the bowel, bladder, ureters, vagina, or rectovaginal septum. DIE can occur at any stage, but is most common at Stage 3 and Stage 4.
What are the symptoms of deep infiltrating endometriosis? DIE symptoms depend on which organ is affected. They are often more severe than superficial endometriosis:
Severe dyschezia — painful bowel movements that can be debilitating, with straining and urgency
Rectal bleeding during menstruation
Severe bladder pain, urgency, and difficulty urinating
Deep sciatic-type nerve pain radiating into the leg or buttock
Chronic constipation or diarrhoea unresponsive to dietary changes
DIE requires advanced imaging before surgery. High-resolution MRI with bowel preparation protocol is the standard for accurate pre-operative mapping. A regular transvaginal ultrasound often misses deep bowel or ureteric disease. Surgery must be done at a specialist centre with a full team. A general gynaecologist should not attempt this.
Adenomyosis vs Endometriosis: How to Tell the Difference
Symptoms for adenomyosis and endometriosis are quite similar. Pelvic pain and severe menstrual periods occur in both cases. Nevertheless, these diseases impact various regions of the body. Women suffer from both disorders simultaneously quite often, which worsens the symptoms and makes the diagnosis harder.
Feature | Endometriosis | Adenomyosis |
What it is | Endometrial-type tissue grows OUTSIDE the uterus | Endometrial tissue grows INTO the uterine muscle wall (myometrium) |
Who it affects | 1 in 10 women of reproductive age (WHO, 2023) | More common in women aged 35-50, often after childbirth |
Uterus size | Normal size unless fibroids co-exist | Typically enlarged and tender |
Main symptoms | Pelvic pain, dyspareunia, infertility, bowel/bladder symptoms (RCOG, 2021) | Heavy, painful periods; pelvic pressure; enlarged uterus (NICE, 2022) |
Diagnosis | Laparoscopy is the gold standard; MRI can suggest deeper lesions | MRI has 80-90% accuracy (ESHRE, 2020); sometimes confirmed by hysterectomy pathology |
Treatment | Excision surgery, hormonal therapy, and hysterectomy in severe cases | Hormonal therapy (Mirena IUS, progestins), uterine artery embolisation, or hysterectomy |
Which Is More Serious, Endometriosis or Adenomyosis?
Neither is more serious than the other — it depends on your case. Endometriosis can affect many organs in the pelvis and abdomen. Stage 4 cases are surgically complex and can seriously threaten fertility. Adenomyosis stays in the uterus. But it can cause just as much pain and very heavy bleeding, with a big impact on quality of life.
If fertility matters to you, endometriosis is usually the bigger concern. It can damage the fallopian tubes and block pathways to the egg. It also makes it hard for an embryo to implant. If your main problem is heavy bleeding and fertility is not a concern, treating adenomyosis — including hysterectomy — often gives the most relief. A specialist assessment is essential before deciding which condition is driving your symptoms.
How Do I Know If I Have Adenomyosis or Endometriosis?
Adenomyosis is suspected from symptoms — heavy, painful periods and an enlarged, tender uterus. It is confirmed by pelvic ultrasound or MRI, which achieves 80-90% accuracy for this condition (ESHRE, 2020). In some cases, confirmation requires a biopsy of the uterine muscle from a hysterectomy specimen.
Endometriosis can be suggested by MRI for deeper lesions. But the gold standard is laparoscopy — a surgical procedure that lets doctors see and biopsy lesions directly. Non-invasive tests are improving but cannot yet replace laparoscopy for definitive staging (It’s About Time, 2024).
You can have both conditions at the same time — this is common. If your imaging shows adenomyosis but you also have deep pain during sex, painful bowel movements, or infertility, your specialist should also check for endometriosis.
What Does Adenomyosis Belly Look Like?
Adenomyosis causes the uterus to grow larger and feel soft and boggy. For some women, this creates visible swelling in the lower abdomen that doesn’t come and go — it stays. Some women describe their belly looking as though they are 3-5 months pregnant, with a firm, tender lower abdomen that doesn’t change through the month (South Lake OBGYN, 2025). This is more pronounced in diffuse adenomyosis, where the whole uterine wall is affected. Without treatment, the swelling can get worse over the years.
Does Adenomyosis Affect the Bowels?
Adenomyosis does not grow on or into the bowel — that is endometriosis. But an enlarged, inflamed uterus can press on nearby bowel structures. This causes bloating, constipation, or a feeling of constant fullness and pressure. Chronic pelvic inflammation also worsens IBS symptoms in many women (NICE, 2022).
If you have adenomyosis and bad bowel symptoms — painful bowel movements, rectal bleeding during your period, or severe dyschezia — ask your specialist to also check for bowel endometriosis. Targeted MRI imaging is the right test.
Can Endometriosis Cause Cancer? What the Research Shows
Endometriosis is not cancer and is not a pre-cancerous condition. It is a benign disease. But long-term research has found a small link between endometriosis and certain types of ovarian cancer. It’s important to understand this clearly — neither dismissing it nor overstating it.
What Cancers Are Linked to Endometriosis?
Two specific subtypes of ovarian cancer have the strongest link to endometriosis:
Clear cell ovarian carcinoma: The strongest association. This subtype of ovarian cancer can develop from endometriotic cysts in some cases.
Endometrioid ovarian carcinoma: Also linked to endometriosis, though less strongly than clear cell.
The general population lifetime risk of ovarian cancer is approximately 1 in 70 (about 1.4%). For women with endometriosis, a 2022 review in The Lancet estimated this risk rises to approximately 1 in 50 (about 2%). That is a small increase in an already uncommon cancer. Most women with endometriosis will never develop ovarian cancer. There is no convincing evidence that endometriosis causes endometrial cancer, cervical cancer, or other cancers.
What Is the Life Expectancy of a Person with Endometriosis?
Endometriosis does not reduce life expectancy. Women with endometriosis live normal lifespans. The small rise in certain ovarian cancer risk does not meaningfully change survival statistics. What endometriosis deeply affect is the quality of life. Chronic pain, mental health burden, reduced work capacity, and relationship impact are all real consequences.
Treating endometriosis through surgery and long-term management is about improving how you live, not how long. Regular check-ups every 1-2 years with your gynaecologist are recommended — especially to monitor known endometriomas.
What Is the New Treatment for Endometriosis (2026)?
In terms of developments regarding endometriosis therapy up until 2026, these can be listed as follows:
GnRH antagonists (Linzagolix, Elagolix): Medications administered orally and do not need injections. They inhibit the production of oestrogen hormone without producing adverse side effects like other GnRH medications. Approved by NICE in recent years for medical management.
Relugolix-combination therapy: A daily oral pill approach combining GnRH antagonism with add-back hormones, increasingly available in the UK and Australia.
Robotic-assisted excision surgery: Provides greater precision for deep infiltrating endometriosis near the bowel and bladder. Available at specialist centres including Apollo Hospitals, Chennai, and Fortis Healthcare, Delhi.
Improved non-invasive diagnostics: The use of serum biomarker research and high-resolution MRIs has led to increased success in non-surgical diagnosis, although laparoscopy continues to be the gold standard for the procedure.
Endometriosis Surgery: What to Expect, Recovery, and Pain Management
Laparoscopy is the most recommended procedure to diagnose and manage endometriosis (NICE, 2017). Excision and ablation can be used based on the level of the condition, its location, fertility plans, and the expertise of the surgeon. Hysterectomy and hormone treatment will depend on similar considerations.
Is Surgery for Endometriosis Major Surgery?
Yes. Even laparoscopic (keyhole) surgery for endometriosis is classified as major surgery (Endometriosis UK, 2022). It requires general anaesthesia and involves internal manipulation of pelvic organs. In complex cases, it carries real risks — including damage to the bowel, bladder, or ureters. The benefits are real: smaller incisions, shorter hospital stay, faster recovery, and less pain than open surgery. But these benefits don’t change how surgery is classified.
For deep infiltrating endometriosis at Stage 3-4, a full team may be needed. That includes a gynaecological surgeon, a colorectal surgeon, and a urologist — all working at the same time. This is why choosing the right centre matters. You need a centre with a dedicated DIE programme and high surgical volume — not a general gynaecologist who does occasional laparoscopies.
Excision vs Ablation: Which Is Better for Endometriosis?
Approach | What It Does | Best For | Recurrence Risk |
Excision | Cuts out the entire lesion including its roots | Deep infiltrating disease, Stage 3-4, any fertility concern | Lower — complete lesion removed |
Ablation (diathermy) | Burns the surface of lesions only | Superficial Stage 1-2 lesions only | Higher — root may remain and regrow |
For most patients, excision surgery is the strongly preferred approach. This is especially true for Stage 2 and above, those with fertility concerns, or those with any deep lesions. Studies consistently show better long-term pain relief and lower recurrence rates than ablation. Ablation is only appropriate for superficial Stage 1 lesions in specific cases. At Divinheal’s partner hospitals, excision is the standard approach.
How Successful Is Endometriosis Surgery?
Laparoscopic excision surgery improves symptoms in over 80% of patients with moderate to severe endometriosis (NICE guidelines; systematic reviews of excision outcomes). For infertility caused by endometriosis, removing lesions and adhesions boosts natural conception rates — especially at Stage 1-3. At Stage 4, surgery combined with IVF gives the best fertility outcomes.
Recurrence is a possibility. The chances of recurrence without any form of post-operative hormonal treatment are about 20 to 30 percent after 5 years. With post-operative hormonal therapy such as oral contraception pills, progestins, or GnRH analogues, the chance of recurrence reduces to only 10 to 15 percent after 5 years. Your surgical team will recommend a hormonal plan that fits your fertility goals.
How Long Does Pain Last After Laparoscopy for Endometriosis?
Recovery timeline after laparoscopic endometriosis surgery:
First 24-48 hours: Abdominal discomfort and shoulder tip pain caused by CO₂ gas during the operation (pain subsides in 24-48 hours due to dissipation of gas). Duration of hospitalization: 1-2 days.
Days 3-7: Gradual improvement. Most patients report pain reducing to manageable levels with prescribed pain relief by day 3-5. Mild fever and fatigue are normal.
Weeks 1-2: You should feel better after 1-2 weeks (myhealth.alberta.ca). Light activities and short walks resume. Avoid driving until off strong pain medicine.
Weeks 2-6: For Stage 3-4 excision, full recovery typically requires 4-6 weeks. Strenuous exercise and sexual intercourse are avoided for 4-6 weeks post-surgery.
Pain after a standard laparoscopy for endometriosis usually resolves within 1-2 weeks. Complex Stage 4 multidisciplinary excision may cause soreness lasting 3-4 weeks. Your Divinheal surgical team will prescribe pain relief and give you a full written recovery plan before you fly home.
What Happens If Endometriosis Is Left Untreated?
If untreated, endometriosis typically gets worse — though not always in a straight line. The consequences of leaving it unmanaged include:
Worsening pain — progressing from cyclical to chronic and constant over the years
Development of ovarian endometriomas can damage egg reserves and reduce ovarian function
Adhesion formation causes organs to bind together — potentially leading to bowel or bladder obstruction in severe cases (Clinton Women’s Healthcare, 2025)
Worsening infertility as adhesions obstruct the fallopian tubes and endometriomas use up the ovarian follicle reserve
A serious psychological component — prevalence of depression and anxiety is significantly higher in untreated women with endometriosis
Living With Endometriosis: Diet, Exercise, and Daily Management
Surgery addresses the disease burden. But management is equally important. You need to employ a series of measures in your life that ensure a reduction in inflammation as well as hormonal balance.
Is Coffee Good for Endometriosis?
Recent research shows no clear link between moderate caffeine and endometriosis rates or severity. Women who drink caffeinated beverages do not have higher rates of endometriosis than non-drinkers (WebMD). But if caffeine worsens your bloating, cramping, or bladder symptoms, switching to decaf is an easy fix. Women with bladder endometriosis often find that caffeine makes urgency and pain worse. Moderate coffee (1-2 cups daily) is generally fine for most women with endometriosis.
Is Running Good for Endometriosis?
Regular moderate exercise is broadly beneficial. It reduces inflammation, improves mood through endorphin release, and can modestly lower oestrogen levels over time. But high-impact running during a flare or your period can make pain worse — especially for Stage 3-4 disease. When pain is well-controlled and you’re not in a flare, running and vigorous exercise are generally fine. During symptomatic periods, lower-impact options — walking, swimming, yoga, or Pilates — are better tolerated and still helpful.
Regular exercise of 30 minutes or more, 3-5 times per week has been linked to a 20-30% reduction in chronic pain severity across multiple chronic pain conditions (WHO, 2020).
How Hard Is It to Live With Endometriosis?
Endometriosis has a huge impact on day-to-day life and emotional well-being. Many women suffer emotional distress, anxiety and depression due to chronic pain, heavy bleeding and fertility challenges. Work, social life and personal relationships often suffer – particularly when the disease is poorly controlled (Raveco, 2025).
Can I live a normal life with endometriosis? Yes — but it takes active management, not passive acceptance. Effective surgery, hormonal management, lifestyle changes, and mental health support all help. Both the NHS and Endometriosis UK recommend patient support groups alongside medical care. Divinheal’s partner hospitals offer physiotherapy and psychological support as part of recovery for international patients.
Endometriosis Treatment Cost in India vs UAE, Australia, and the UK
India offers the same JCI-accredited endometriosis surgery as UAE, Australia, and UK private hospitals — at 55-75% less cost. The difference is in running costs, not medical quality.
Cost Comparison: Endometriosis Surgery in India vs Source Countries
Country | Laparoscopic Excision (incl. 2-night hospital stay) | Savings vs India |
India | INR 1,80,000 - 3,50,000 ($2,150 - $4,200 / AUD 3,200 - 6,300 / AED 7,900 - 15,400 / GBP 1,700 - 3,300) | — |
UAE | AED 15,000 - 35,000 ($4,080 - $9,530) | Save 55-70% |
Australia | AUD 8,000 - 15,000 ($5,200 - $9,800) | Save 55-70% |
UK (private) | GBP 5,000 - 12,000 ($6,300 - $15,100) | Save 60-75% |
India (Hysterectomy, if required) | INR 3,00,000 - 5,50,000 ($3,600 - $6,600 / AUD 5,400 - 9,900 / AED 13,200 - 24,200 / GBP 2,850 - 5,150) | — |
All estimates are based on the range of private healthcare as of 2026. Both the NHS (UK) and Medicare (AU) can pay for the service, but there are considerable wait times involved. The actual cost depends on the level of the hospital, the complexity of the staging (Stage 4 surgery is more complex), and whether or not a hysterectomy is needed. Costs are approximate and depend on hospital, surgeon seniority, and case complexity.
Why Choose India for Endometriosis Surgery?
India’s lower costs come from cheaper running costs and property, not lower quality. High surgical volume builds deep expertise. A domestic drug industry keeps medication costs much lower than in Western markets. Here are the key advantages for endometriosis patients:
Specialist surgical volume: Leading centres such as Apollo Hospitals, Chennai perform 1,000+ gynaecological laparoscopies annually. Surgical expertise is directly linked to case volume — especially for complex Stage 4 and DIE excision.
No wait-list: UK NHS referral to specialist gynaecologist averages 6-18 months; Australian specialist wait times are typically 3-12 months. Divinheal arranges a consultation within 5-10 working days.
Multidisciplinary DIE teams: Stage 4 and deep infiltrating cases require colorectal and urological input at the same time. India’s partner hospitals have these teams in-house — not guaranteed at general gynaecology clinics in the UK or Australia.
JCI and NABH accreditation: Over 40 Indian hospitals hold Joint Commission International accreditation — equivalent to the standards of UK and Australian private hospitals.
Arabic-speaking coordinators: For UAE patients, dedicated coordinators at partner hospitals ensure clear communication and cultural comfort, including halal meal options and prayer facilities.
Key Partner Hospitals for Endometriosis in India
Hospital | Location | Accreditation | Speciality |
Apollo Hospitals | Chennai | JCI, NABH | Gynaecological laparoscopy, DIE, fertility surgery, robotic excision |
Fortis Healthcare | Delhi | JCI, NABH | Complex Stage 4 excision, multidisciplinary DIE team, robotic surgery |
Max Healthcare | Delhi | JCI, NABH | Multidisciplinary gynaecology, endometriosis, bowel endometriosis |
Artemis Hospital | Gurugram | JCI, NABH | Advanced laparoscopic surgery, women’s health centre |
Aster CMI Hospital | Bengaluru | JCI, NABH | Women’s health, DIE, fertility, international patient services |
These are illustrative composites of stories based on the experience of typical patients. Patient names have been withheld to ensure confidentiality. Results can vary from person to person. Please contact your specialist for further advice.
Quick Answer — At a Glance
Skim this if you’re short on time.
Endometriosis: Key Facts for 2026 — At a Glance
|
Related Links
International Patient Visiting India
- ivf in bengaluru for ethiopia
- ivf in pune for bangladesh
- ivf in mumbai for bangladesh
- ivf in bengaluru for bangladesh
- ivf in pune for uae
- ivf in bengaluru for uae
- ivf in new delhi for uae
- ivf in hyderabad for uae
- ivf in chennai for bangladesh
- ivf in new delhi for iraq
- ivf in bengaluru for iraq
- ivf in mumbai for iraq
- ivf in chennai for iraq
- ivf in bengaluru for nigeria
- ivf in pune for nigeria
- ivf in hyderabad for nigeria
- ivf in new delhi for ethiopia
- ivf in hyderabad for bangladesh
- ivf in mumbai for uae
- ivf in pune for iraq
Booking With DIVINHEAL
Get a free consultation to understand your treatment options
Related Links
International Patient Visiting India
- ivf in bengaluru for ethiopia
- ivf in pune for bangladesh
- ivf in mumbai for bangladesh
- ivf in bengaluru for bangladesh
- ivf in pune for uae
- ivf in bengaluru for uae
- ivf in new delhi for uae
- ivf in hyderabad for uae
- ivf in chennai for bangladesh
- ivf in new delhi for iraq
- ivf in bengaluru for iraq
- ivf in mumbai for iraq
- ivf in chennai for iraq
- ivf in bengaluru for nigeria
- ivf in pune for nigeria
- ivf in hyderabad for nigeria
- ivf in new delhi for ethiopia
- ivf in hyderabad for bangladesh
- ivf in mumbai for uae
- ivf in pune for iraq
Meet Our Doctors
Meet our team of highly qualified and experienced medical professionals dedicated to providing the best healthcare services.

Dr Aditi Dixit
Sr. Consultant – Women Imaging
Radiology
New Delhi
15+ Years
Experience
Artemis Hospital
Hospital
1500
Fees

Dr. Alka Gujral
Senior Consultant
Obstetrics and Gynaecology
New Delhi
24+ Years
Experience
Apolo Delhi
Hospital
1500
Fees

Dr. Anita K. Sharma
Senior Consultant - Obstetrics and Gynaecology
Obstetrics and Gynaecology
New Delhi
24+ Years
Experience
Apolo Delhi
Hospital
1500
Fees

Dr. Anjali Bhutani
Senior Consultant
Obstetrics & Gynaecology
New Delhi
22+ Years
Experience
Apolo Delhi
Hospital
1500
Fees

Dr. Aparna Dhar
Senior Consultant - Obstetrics & Gynaecology
Obstetrics & Gynaecology
New Delhi
23+ Years
Experience
Apolo Delhi
Hospital
1500
Fees

Dr. Babita Jain
Principal Director & HOD
Paediatrics (Ped)
New Delhi
30+ Years
Experience
Max Hospital,Gurgaon
Hospital
1500
Fees

Dr Chandrima Misra M
Co-Head Psychological Services
Mental Health and Behavioural Sciences
New Delhi
15+ Years
Experience
Artemis Hospital
Hospital
1500
Fees

Dr. Charu Garg
Principal Director - Radiation Oncology
Radiation Oncology
New Delhi
23+ Years
Experience
Max Hospital,Gurgaon
Hospital
1500
Fees

Dr. Gyanendra Agrawal
Director - Obstetrics & Gynaecology
Obstetrics & Gynaecology
New Delhi
18+ Years
Experience
Apolo Delhi
Hospital
1500
Fees

Dr. Kanika Gupta
Principal Director – Surgical Oncology (Gynae & Robotic Surgery)
Gynecologic Oncology, Robotic & Laparoscopic Surgery, Gynae Cancer Care, Surgical Oncology
New Delhi
39+ Years
Experience
Max Hospital,Gurgaon
Hospital
1500
Fees
DivinHeal's Journey

Latest Articles




Hospitals Offering this treatment
India offers premium medical procedures at affordable prices. Discover our most popular treatments, delivered by the country's finest doctors.

Hisar Intercontinental Hospital
Saray Mah. Siteyolu Cad. No:7, Umraniye, 34768, Istanbul, Turkey
Hisar Intercontinental Hospital

Medical Park Group, Istanbul
Fahrettin Kerim Gokay Cad. Tıbbiye Cd., Kadikoy, Istanbul, Turkey
Medical Park Group, Istanbul

Emsey Hospital, Pendik, Istanbul
Çamlık, Selçuklu Cd. No:22, 34912 Pendik/İstanbul, Türkiye
Emsey Hospital, Pendik, Istanbul


American Hospital, Istanbul
Guzelbahce Sk. No:20, 34365, Nisantasi, Istanbul, Turkey
American Hospital, Istanbul

Memorial Hospitals Group
Burhaniye, Nagehan Sokağı No:4/A D:1, 34676 Üsküdar/İstanbul, Türkiye
Memorial Hospitals Group

Florence Nightingale Hospital Istanbul
Abide-i Hürriyet Cd No:166, 34381 Sisli, Istanbul
Florence Nightingale Hospital Istanbul

Medicana International Hospital, Istanbul
Halit Ziya Turkkani Mah. Medikal Park Cd. No:1, Beylikdüzü, İstanbul
Medicana International Hospital, Istanbul

Okan University Hospital Istanbul
Icmeler Mah. Aydınlıyolu Cd. No:2, 34947 Icmeler-Tuzla, Istanbul
Okan University Hospital Istanbul

Kolan International Hospital, Istanbul
Kaptanpasa Mah. Okmeydan Kavsagi, Darulaceze Cd. No:14, 34384 Sisli, Istanbul
Kolan International Hospital, Istanbul
Frequently Asked Questions
Get answers to common questions about medical tourism, treatment procedures, and our comprehensive healthcare services.
Ready To Start Your Healing Journey?
Get Personalized Medical Treatment Options From India's Top Hospitals. Our Medical Experts Are Ready To Assist You Every Step Of The Way.