
Written by DivinHeal Editorial Contributor, Samrat Nilesh, Embryologist | Medically Reviewed by Dr Indu Priya, Gynecologist(MBBS,MD) Published on: 2026-05-17
Why Am I Not Ovulating But Having Periods? Ovulation Tests, Pain, Cramps & Anovulation Treatment in India
Having periods but not ovulating is called anovulation. It is one of the most common reasons people have trouble getting pregnant. It is also very misunderstood. Regular-looking periods do not mean an egg was released. This guide explains what ovulation tests look for and why ovulation pain happens. It also covers what causes anovulation and what the treatment costs in India are for patients from Nigeria, Australia, and the UK.
Understanding Ovulation: Signs, Pain, and What Your Body Is Telling You
What Are the 7 Signs of Ovulation?
Ovulation happens once each menstrual cycle. It usually occurs 12–16 days before your next period. The seven most reliably recognised signs of ovulation are:
Change in cervical mucus — as ovulation gets close, cervical mucus becomes more abundant, clear, slippery, and stretchy. It looks like raw egg white. This is the most useful natural sign of fertility.
LH surge detected by ovulation test — a positive ovulation predictor kit (OPK) detects the LH surge. This surge happens 24–36 hours before the egg is released.
Mid-cycle pain or cramping (Mittelschmerz) — mild to moderate one-sided lower abdominal pain during ovulation. It usually lasts a few minutes to 2 days. It happens when the follicle breaks open and releases the egg.
Basal body temperature (BBT) rise — after ovulation, progesterone raises your resting body temperature by about 0.2–0.5°C (0.4–1.0°F). This rise lasts until your next period.
Light mid-cycle spotting — a small amount of light pink or brown spotting can happen when the follicle breaks open. This does not happen in all women.
Breast tenderness — hormone changes around ovulation can make your breasts or nipples feel mildly sensitive.
Increased libido and heightened senses — oestrogen peaks just before ovulation. This is linked to a higher sex drive and a sharper sense of smell in some women.
The most reliable way to confirm ovulation is to use multiple signs together. Look at cervical mucus changes, a positive OPK, and the BBT rise. One sign on its own is not enough.
How Do I Know If I’m Ovulating?
The most accessible methods to confirm ovulation:
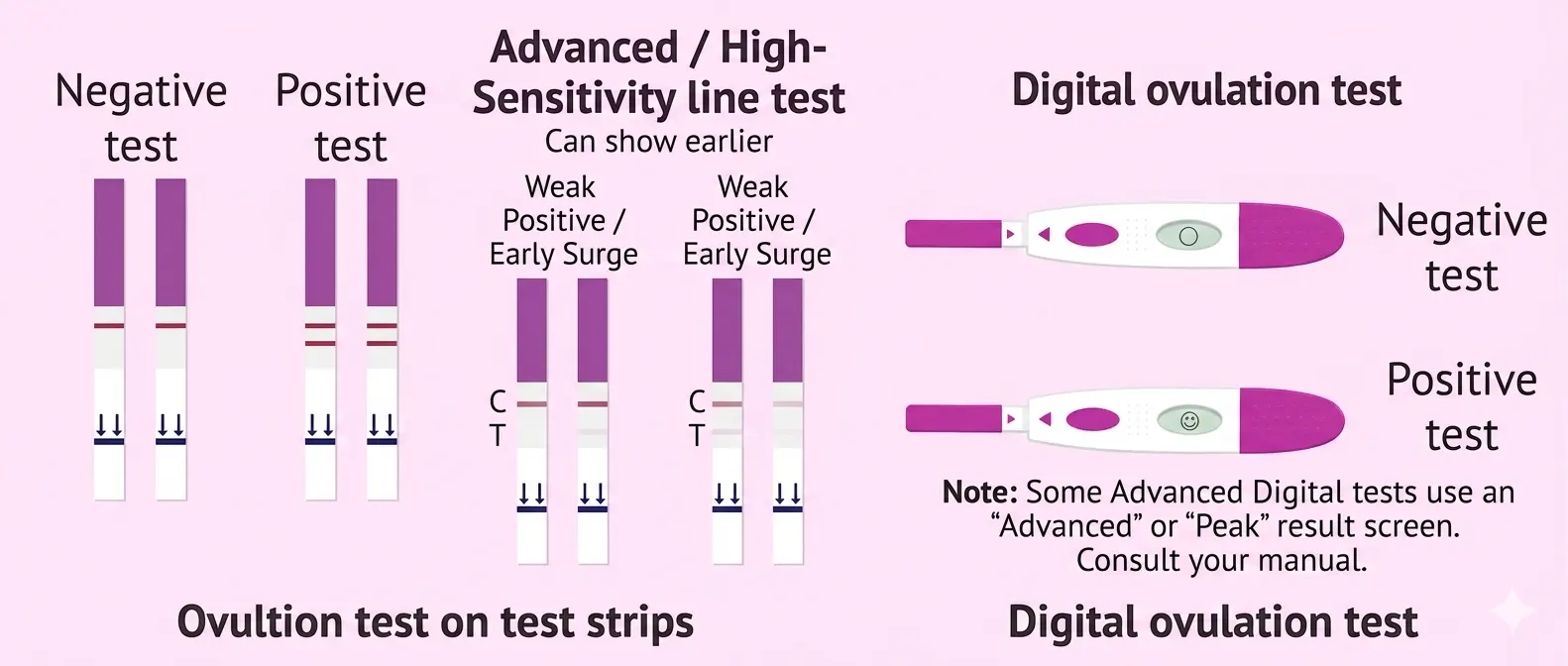
Ovulation predictor kits (OPKs) — detect the LH surge 24–36 hours before ovulation. A positive test means the test line is as dark as or darker than the control line. This means the egg will be released very soon. You can buy OPKs at pharmacies in Nigeria, Australia, and the UK. Start testing a few days before your expected ovulation. For a 28-day cycle, start from day 10 or 11.
Basal body temperature (BBT) charting — take your temperature with a digital thermometer every morning before getting up. A rise of 0.2–0.5°C that lasts for 3+ days confirms ovulation has likely happened.
Cervical mucus monitoring — check the feel of your mucus daily. Egg-white mucus is a sign of peak fertility. It becomes dry again after ovulation as progesterone rises.
Progesterone blood test — this test is taken 7 days after suspected ovulation (day 21 of a 28-day cycle). It is the most reliable non-invasive way to confirm ovulation. A result above 16–30 nmol/L confirms it occurred. The exact threshold depends on the laboratory.
Follicle tracking ultrasound — a series of transvaginal ultrasounds through the cycle. A specialist watches the follicle grow. Then they confirm whether the follicle breaks open. This is the gold standard for confirming ovulation.
How Ovulation Tests Work: Kits, Timing, and Accuracy
What Ovulation Tests Detect: LH Surge Explained
Ovulation predictor kits detect the luteinising hormone (LH) in your urine. The pituitary gland makes LH. It peaks 24 to 36 hours before the ovary releases an egg. The test strip has antibodies that attach to LH. When the LH level is high enough, a coloured line appears. A positive result is when the test line is as dark as or darker than the control line. This means an LH surge is happening. Ovulation likely to occur in 24-36 hours.
Digital OPKs show ‘high’ or ‘peak’ fertility. ‘Peak’ means the LH surge has started. Advanced OPKs (Clearblue Advanced, for example) also detect the rise in oestrogen before the LH surge. This gives you an extra day or two of ‘high’ fertility warning before the peak.
When and How to Use an Ovulation Test Correctly
Follow these steps for the best results:
Start testing a few days before your expected ovulation. For a 28-day cycle, start around day 10 or 11. For longer cycles, subtract 17 from your cycle length to find your start day.
Test at the same time each day. Late morning to early afternoon works best for standard LH tests. Avoid first morning urine — LH builds up overnight and may not show in urine early in the morning. Pregnancy tests are different; those use first morning urine.
Do not drink too many fluids for 2 hours before testing. Diluted urine can give a false negative.
Read results within the timeframe in the kit instructions (usually 5–10 minutes). Lines that appear after this window may not be reliable.
Interpreting a Positive Ovulation Test: What to Do Next
A positive ovulation test means LH has surged. Ovulation is likely within 12–36 hours. This is the peak of your fertile window. If you are trying to conceive, have intercourse on the day of the positive test and the day after. Your fertile window starts about 5 days before ovulation and ends on the day of ovulation. Intercourse in the days before a positive test is also fertile. Sperm can survive up to 5 days in the reproductive tract. The egg survives only 12–24 hours after release.
Limitations of Ovulation Tests: When You Don’t Get a Positive
If you keep getting negative ovulation tests, there are a few possible reasons. There may be no LH surge at all (anovulation). The surge may happen too briefly for the test to catch. The surge may happen outside the testing window — often early in the morning. Less commonly, LH levels may be very low. In women with PCOS, the opposite can happen. LH levels stay high all the time. This causes the test to look positive even when there is no true surge. An ovulation test alone cannot confirm anovulation. You need a specialist to assess this.
Ovulation Pain (Mittelschmerz): Causes, Signs, and What It Means
What Is Ovulation Pain? Understanding Mittelschmerz
Mittelschmerz (from German: ‘middle pain’) is the medical term for one-sided lower abdominal pain during ovulation. About 20% of women feel this pain during their reproductive years (Cleveland Clinic). It happens because the dominant follicle — a fluid-filled sac holding the egg — swells and then breaks open. This can briefly irritate the abdominal lining (peritoneum), causing pain or cramping. The pain is usually on the side of the ovulating ovary. It can switch sides each cycle, though some women ovulate from one ovary more often.
Mittelschmerz is a sign that ovulation is happening on that side. But not feeling pain does not mean you are not ovulating. Many women ovulate without any pain at all.
Is Ovulation Pain Normal? How Long Does It Last?
Yes — Mittelschmerz is a normal body event. It goes away on its own in most cases. It lasts from a few minutes to 2 days. It can feel like a mild, dull ache or a brief, sharp twinge. Most women who have it learn to spot it as a monthly mid-cycle pattern. It does not need medical treatment unless it is severe, lasts a long time, or comes with other symptoms that point to another condition.
Ovulation Cramps vs Period Cramps vs Implantation Cramps
Feature | Ovulation Cramps | Menstrual Period Cramps | Implantation Cramps |
Timing | Mid-cycle (around day 14 of 28-day cycle) | Start of period; days 1–3 typically | 6–12 days after ovulation |
Location | One side only (left or right) — the ovulating ovary side | Lower abdomen, diffuse, often radiating to the lower back | Lower abdomen, mild and localised |
Intensity | Mild to moderate; dull ache or sharp twinge | Moderate to severe; often the most intense of the three | Mild; sometimes described as fluttering or pressure |
Duration | Minutes to 1–2 days | 3–7 days alongside the period | A few hours to 2–3 days |
Associated symptoms | Sometimes light spotting (Mittelschmerz), bloating, or a brief discharge change | Heavy bleeding, clots, lower back pain, nausea | Light spotting; breast tenderness; no period |
Does Ovulation Pain Mean the Egg Has Been Released?
Ovulation pain happens around the time the follicle breaks open, and the egg is released. But the timing is not exact. Pain can start while the follicle is still growing — before it breaks open. It can also continue briefly after. The pain alone cannot tell you the egg was released at that exact moment. The most reliable ways to confirm egg release are: a progesterone blood test 7 days after expected ovulation — a high result means ovulation happened; or a follicle tracking ultrasound. The ultrasound shows a collapsed follicle and free fluid, which are both signs of rupture.
Is Ovulation Pain Too Late to Conceive?
Not necessarily. When Mittelschmerz pain starts, ovulation may still be happening — the follicle may be breaking open or have just opened. The egg survives for 12–24 hours after release. If you feel ovulation pain and have intercourse that same day, the egg may still be viable. Sperm can fertilise the egg if they reach the fallopian tube in time. However, having intercourse in the days before the pain is more reliable. Sperm can survive up to 5 days in the reproductive tract. They can wait there for the egg to be released.
What Helps Ovulation Cramps?
For most women, ovulation cramps are mild and go away quickly. Effective relief options include:
over-the-counter pain relief (paracetamol or ibuprofen) taken at the start of pain
a warm compress or heat pad on your lower abdomen
gentle movement or a warm bath
drinking enough water
Use ibuprofen with care if you are trying to conceive during your fertile window. Some evidence shows NSAIDs may affect follicle rupture at high doses in some women. Talk to your GP if this concerns you.
When Ovulation Pain Could Signal a Problem
See a doctor if your ovulation pain is severe or lasts more than 2–3 days. Also see a doctor if the pain is getting worse, or if it comes with fever, vomiting, or unusual discharge. Pain during intercourse is also a warning sign. These features can point to:
ovarian cysts, which can mimic or worsen Mittelschmerz
endometriosis — ovarian endometriomas are linked to more intense mid-cycle pain
pelvic inflammatory disease
Rarely, ovarian torsion — twisting of the ovary, which is a medical emergency
A pelvic ultrasound and specialist review can identify these conditions.
Why Am I Not Ovulating But Having Periods? Understanding Anovulation
What Is Anovulation and Why Does It Happen?
Anovulation is when the ovaries do not release an egg during a menstrual cycle. Even without ovulating, many women with anovulation still bleed. Doctors call this withdrawal bleeding. Oestrogen changes drive it — not the rise in progesterone that follows true ovulation. The bleeding may be irregular, lighter, heavier, or at odd intervals. But it can also look fairly normal. That is why anovulation often goes unnoticed until someone has trouble getting pregnant.
Ovulation should be regulated by a precise hormonal cycle. To start, the hypothalamus produces GnRH. GnRH stimulates the pituitary to secrete FSH. FSH promotes follicular growth. After that, the pituitary secretes LH. LH stimulates ovulation. Any interference with this process causes anovulation.
Common Causes of Anovulation
Polycystic Ovary Syndrome (PCOS) is the most common cause of anovulatory infertility. It accounts for approximately 70–85% of such cases (ACOG). PCOS disrupts LH and FSH signals. This stops follicles from maturing and prevents ovulation.
Thyroid disorders — both hypothyroidism and hyperthyroidism can upset the hormone balance needed for ovulation. The thyroid hormone affects how GnRH is released.
Hyperprolactinaemia — this means high prolactin levels. It can come from pituitary tumours, certain medications, or thyroid disease. High prolactin suppresses GnRH and can prevent ovulation.
Significant weight changes — being underweight can reduce oestrogen. Being overweight can produce too much oestrogen and androgens. Both can cause anovulation.
Excessive exercise or athletic training — common in competitive athletes. Very low energy intake can suppress the HPO axis and stop ovulation.
Chronic stress — long-term high cortisol can suppress GnRH and stop ovulation.
Perimenopause — as ovarian reserve drops before menopause, cycles become more and more anovulatory.
Premature ovarian insufficiency (POI) — ovarian failure before age 40. A smaller follicle pool leads to high FSH and anovulation.
How Anovulation Is Diagnosed
Tests used to check for anovulation:
Hormone blood panel — tests FSH, LH, AMH, prolactin, thyroid (TSH, free T4), oestradiol, and day-21 progesterone. Low progesterone on day 21 points to anovulation. If PCOS is suspected, androgens (testosterone, DHEAS) are also tested.
Follicle tracking ultrasound — a transvaginal scan done through the mid-cycle. A specialist watches the follicle grow. They check whether it breaks open. This is the gold standard for confirming anovulation.
Ovarian reserve assessment — uses AMH level and antral follicle count (AFC). An early cycle scan shows how much ovarian reserve you have.
Hysterosalpingography (HSG) — a dye study of the fallopian tubes and uterus. It checks for tubal blockage if that is also a concern.
At NABH/JCI-accredited partner hospitals in Delhi NCR and Chennai, the full diagnostic workup can be done within 1–2 weeks of arrival. It includes hormone panels, follicle tracking scans, and an ultrasound.
Anovulation Treatment in India: Options and Costs
Ovulation Induction: Medical Treatment for Anovulation
The main medical treatment for anovulation is ovulation induction. This uses medicine to help the ovaries produce and release an egg:
Clomiphene citrate (Clomid) — the most used first-line oral treatment. It prompts the pituitary to make more FSH and LH. This helps follicles grow. It works in approximately 70–80% of women with PCOS-related anovulation. Pregnancy rates per cycle are 15–20% (multiple published meta-analyses). It is used for 3–6 cycles.
Letrozole (Femara) — now preferred over Clomiphene for PCOS-related anovulation. It gives higher live birth rates in PCOS patients in randomised trials (NEJM, Legro et al., 2014). It also carries a lower risk of multiple pregnancy.
Injectable gonadotropins — FSH or FSH/LH injections for patients who do not respond to oral agents. These are more potent. They need careful monitoring with scans and blood tests to prevent ovarian hyperstimulation syndrome (OHSS).
Metformin (for PCOS with insulin resistance) — this can restore ovulation in some PCOS patients. It is often used alongside Letrozole.
All ovulation induction cycles at partner hospitals are monitored with serial scans. This tracks follicle growth and helps prevent multiple pregnancies or OHSS.
Advanced Reproductive Technologies for Anovulation
Ovulation induction is tried over 3–6 cycles. If pregnancy does not happen — or if there are other fertility factors like male factor, tubal disease, or prior endometriosis surgery — the next steps are:
Intrauterine Insemination (IUI) with ovulation induction — doctors place prepared sperm directly into the uterus at the time of monitored ovulation. Per-cycle success rates are 10–20% depending on age and diagnosis.
In Vitro Fertilisation (IVF) — doctors collect eggs after ovarian stimulation and fertilise them in a laboratory. The embryos are then placed in the uterus. Per-cycle success rates for women under 35 are approximately 40–50%. For women aged 35–39, the rate is 30–40% (HFEA data).
IVF with egg freezing — this helps women preserve their fertility. It is useful before treating anovulation or before hormonal or surgical treatment.
Cost of Anovulation Treatment: India vs Nigeria, Australia, and UK
The table below shows costs for all major fertility services at Divinheal partner hospitals. Prices are shown in NGN, AUD, and GBP.
Treatment Component | India (INR / USD) | Australia (AUD) | UK (GBP) | Nigeria (NGN approx.) |
Specialist fertility consultation | ₹2,000–₹7,000 ($25–$85; AUD 38–130; £23–£80) | AUD 200–500 | £150–£400 | NGN 40,000–140,000 |
Hormone blood panel (FSH, LH, AMH, prolactin, thyroid) | ₹8,000–₹20,000 ($96–$240; AUD 148–370; £91–£229) | AUD 200–400 | £150–£350 | NGN 160,000–330,000 |
Follicle tracking ultrasound (transvaginal) | ₹3,000–₹8,000 ($36–$96; AUD 55–148; £34–£91) | AUD 150–300 | £100–£250 | NGN 60,000–160,000 |
Ovulation induction — oral (Clomiphene/Letrozole, per cycle with monitoring) | ₹15,000–₹30,000 ($180–$360; AUD 278–555; £171–£343) | AUD 2,500–5,000 | £1,500–£3,500 | NGN 300,000–500,000 |
Ovulation induction — injectable gonadotropins (per cycle with monitoring) | ₹40,000–₹80,000 ($480–$960; AUD 740–1,480; £457–£914) | AUD 5,000–12,000 | £3,000–£7,000 | NGN 800,000–1,600,000 |
IVF — single cycle (all-inclusive estimate) | ₹1,20,000–₹2,50,000 ($1,440–$3,000; AUD 2,220–4,625; £1,371–£2,857) | AUD 10,000–20,000 | £5,000–£12,000 | NGN 2,400,000–5,000,000 |
Sources: Apollo Hospitals Chennai, Fortis Noida, Medanta Gurgaon, MAX Hospitals, Artemis Gurgaon, Paras Hospitals (India partner hospital direct pricing). Australia: private fertility clinic published tariffs 2025. UK: HFEA-registered clinic fee ranges 2024–25. Nigeria: a major Lagos private fertility clinic estimates 2025. Currency conversions at Q1 2026 rates (1 AUD ≈ 54.5 INR; 1 GBP ≈ 105 INR; 1 USD ≈ 83.5 INR; 1 USD ≈ 1,650 NGN). All figures approximate private-pay ranges; individual costs depend on treatment complexity and length of stay.
Divinheal’s Partner Hospitals for Fertility Care in India
Divinheal works with NABH/JCI-accredited partner hospitals in Delhi NCR and Chennai. These hospitals have dedicated fertility departments. All hospitals offer anovulation diagnosis, ovulation induction, IUI, and IVF. Many use ART technology that meets HFEA (UK) and Fertility Society of Australia standards.
Hospital | City | Accreditation | Fertility & Ovulation Services |
Apollo Hospitals Chennai | Chennai | JCI, NABH | Fertility consultations; anovulation diagnosis (hormone panels, follicle tracking); ovulation induction; IUI and IVF; international patient centre with English and Arabic support |
Fortis Hospital Noida | Delhi NCR | NABH | Gynaecology and fertility; anovulation assessment; ovulation induction; follicle tracking ultrasound; IUI and IVF referrals within the Fortis network |
Medanta Gurgaon | Gurgaon (Delhi NCR) | JCI, NABH | Comprehensive reproductive medicine; anovulation and PCOS management; IVF and ART; 3D/4D ultrasound diagnostics; international patient wing |
MAX Hospitals | Delhi NCR | NABH | Fertility and reproductive endocrinology; anovulation workup; ovulation induction; IUI and IVF; genetic screening for fertility |
Artemis Gurgaon | Gurgaon (Delhi NCR) | JCI, NABH | Gynaecology and fertility consultations; anovulation diagnosis; ovulation induction; international patient coordination, including Nigerian patient support |
Paras Hospitals | Gurgaon (Delhi NCR) | NABH | Gynaecology; anovulation and fertility assessment; ovulation induction; cost-accessible NABH-accredited care for Nigerian, Australian and UK patients |
The Divinheal medical team confirms specialist details before matching. Medanta Gurgaon and MAX Hospitals have the highest IVF volumes in Delhi NCR. Apollo Hospitals Chennai is the top choice for UAE and African patients who need Arabic-speaking support. Contact Divinheal for current specialist availability.
Planning Your Fertility Treatment Trip to India
Aspect | Nigeria | Australia | UK |
Visa type | Indian Medical Visa via High Commission Lagos or Abuja | Indian Medical e-Visa (online) | Indian Medical Visa via VFS Global |
Processing | 7–21 business days; apply 4 weeks before travel | 5–10 business days | 10–15 working days |
Typical flight | Lagos (LOS) → Delhi (DEL): ~10–12 hrs via Dubai, Doha, or Addis Ababa | Sydney/Melbourne → Delhi: ~12–13 hrs | London Heathrow → Delhi: ~8.5 hrs |
Recommended stay | 14–21 days for full anovulation workup + first treatment cycle | 14–21 days for full workup + first treatment cycle | 10–14 days for initial consultation + first cycle |
Divinheal gives you the hospital invitation letter you need for your Medical Visa. For Nigerian patients, Divinheal advises on the exact letter format needed by the Indian High Commission in Lagos and Abuja.
How Divinheal Supports Nigerian, Australian, and UK Fertility Patients
Pre-travel specialist review — upload your hormone test results, ultrasound reports, and clinical history. A named fertility specialist at the partner hospital will give you a written treatment plan. You will receive a cost estimate in NGN, AUD, or GBP before you commit to travel.
Specialist matching based on your anovulation cause, treatment type (oral induction vs injectable vs IVF), and budget.
Appointment booking within 1–2 weeks of enquiry.
Indian Medical Visa invitation letter for all nationalities.
Accommodation near the partner hospital (1–2 km; serviced apartments at ₹3,000–₹7,000 per night — approximately AUD 55–130; £29–£67; USD 36–84).
Airport transfers on arrival and departure; in-city transport for monitoring appointments.
Post-return telemedicine follow-up with the treating fertility specialist.
Written discharge summary for your home-country gynaecologist or GP.
Divinheal does not charge a placement fee. Partner hospital rates are direct patient pricing. Written cost estimates in NGN, AUD, or GBP are provided before any travel commitment.
Adaeze, a 34-year-old from Lagos (illustrative composite, name changed), had been trying to conceive for 2 years. She was diagnosed with PCOS-related anovulation. A Lagos private fertility clinic quoted approximately NGN 600,000 per cycle. She uploaded her hormone panel through Divinheal. A specialist at Artemis Gurgaon confirmed that Letrozole induction with monitoring was right for her case. She completed her first monitored cycle in India. Total cost in India — including consultation, monitoring, and medication — was approximately USD 350 (NGN 577,000). She returned home with a progesterone result, a detailed cycle report, and a telemedicine follow-up booked.
The story is an illustrative composite based on typical patient journeys. Name changed for privacy. All costs are approximate.
Final Thoughts
Anovulation — not ovulating despite having periods — is one of the most treatable causes of fertility problems. The cause may be PCOS, a thyroid condition, prolactin imbalance, or hormone disruption from weight changes. Effective diagnosis and treatment exist for all of these. Ovulation induction with Letrozole or Clomiphene works in the majority of suitable candidates. IUI and IVF offer further options when needed.
Women from Nigeria, Australia, and the UK often face long waits or high costs at home. NABH/JCI-accredited partner hospitals in Delhi NCR and Chennai offer specialist fertility care. Costs are 60–85% lower than those in private clinics in Australia or the UK. Costs are also competitive with Nigerian private fertility clinics, with higher treatment volumes and better technology. Contact Divinheal for a free case review. A specialist will check your hormone results before you travel. You will get a written cost estimate in NGN, AUD, or GBP before any travel commitment.
Medical disclaimer: All information in this article is for learning purposes only. It is not medical advice. Anovulation and fertility treatment need a specialist evaluation. All decisions should be made with a qualified gynaecologist or reproductive endocrinologist who has reviewed your case. Cost figures are approximate 2025–2026 estimates at NABH/JCI-accredited partner hospitals. Currency conversions at Q1 2026 rates. Individual outcomes vary.
Related Links
International Patient Visiting India
- ivf in bengaluru for ethiopia
- ivf in pune for bangladesh
- ivf in india for bangladesh
- ivf in mumbai for bangladesh
- ivf in bengaluru for bangladesh
- ivf in pune for uae
- ivf in bengaluru for uae
- ivf in new delhi for uae
- ivf in hyderabad for uae
- ivf in chennai for bangladesh
- ivf in new delhi for iraq
- ivf in bengaluru for iraq
- ivf in mumbai for iraq
- ivf in chennai for iraq
- ivf in bengaluru for nigeria
- ivf in pune for nigeria
- ivf in hyderabad for nigeria
- ivf in india for nigeria
- ivf in india for ethiopia
- ivf in new delhi for ethiopia
Booking With DIVINHEAL
Get a free consultation to understand your treatment options
Related Links
International Patient Visiting India
- ivf in bengaluru for ethiopia
- ivf in pune for bangladesh
- ivf in india for bangladesh
- ivf in mumbai for bangladesh
- ivf in bengaluru for bangladesh
- ivf in pune for uae
- ivf in bengaluru for uae
- ivf in new delhi for uae
- ivf in hyderabad for uae
- ivf in chennai for bangladesh
- ivf in new delhi for iraq
- ivf in bengaluru for iraq
- ivf in mumbai for iraq
- ivf in chennai for iraq
- ivf in bengaluru for nigeria
- ivf in pune for nigeria
- ivf in hyderabad for nigeria
- ivf in india for nigeria
- ivf in india for ethiopia
- ivf in new delhi for ethiopia
Meet Our Doctors
Meet our team of highly qualified and experienced medical professionals dedicated to providing the best healthcare services.

Dr Aditi Dixit
Sr. Consultant – Women Imaging
Radiology
New Delhi
15+ Years
Experience
Artemis Hospital
Hospital
1500
Fees

Dr. Alka Gujral
Senior Consultant
Obstetrics and Gynaecology
New Delhi
24+ Years
Experience
Apolo Delhi
Hospital
1500
Fees

Dr. Anita K. Sharma
Senior Consultant - Obstetrics and Gynaecology
Obstetrics and Gynaecology
New Delhi
24+ Years
Experience
Apolo Delhi
Hospital
1500
Fees

Dr. Anjali Bhutani
Senior Consultant
Obstetrics & Gynaecology
New Delhi
22+ Years
Experience
Apolo Delhi
Hospital
1500
Fees

Dr. Aparna Dhar
Senior Consultant - Obstetrics & Gynaecology
Obstetrics & Gynaecology
New Delhi
23+ Years
Experience
Apolo Delhi
Hospital
1500
Fees

Dr. Babita Jain
Principal Director & HOD
Paediatrics (Ped)
New Delhi
30+ Years
Experience
Max Hospital,Gurgaon
Hospital
1500
Fees

Dr Chandrima Misra M
Co-Head Psychological Services
Mental Health and Behavioural Sciences
New Delhi
15+ Years
Experience
Artemis Hospital
Hospital
1500
Fees

Dr. Charu Garg
Principal Director - Radiation Oncology
Radiation Oncology
New Delhi
23+ Years
Experience
Max Hospital,Gurgaon
Hospital
1500
Fees

Dr. Gyanendra Agrawal
Director - Obstetrics & Gynaecology
Obstetrics & Gynaecology
New Delhi
18+ Years
Experience
Apolo Delhi
Hospital
1500
Fees

Dr. Kanika Gupta
Principal Director – Surgical Oncology (Gynae & Robotic Surgery)
Gynecologic Oncology, Robotic & Laparoscopic Surgery, Gynae Cancer Care, Surgical Oncology
New Delhi
39+ Years
Experience
Max Hospital,Gurgaon
Hospital
1500
Fees
DivinHeal's Journey

Latest Articles







Hospitals Offering this treatment
India offers premium medical procedures at affordable prices. Discover our most popular treatments, delivered by the country's finest doctors.

Hisar Intercontinental Hospital
Saray Mah. Siteyolu Cad. No:7, Umraniye, 34768, Istanbul, Turkey
Hisar Intercontinental Hospital

Medical Park Group, Istanbul
Fahrettin Kerim Gokay Cad. Tıbbiye Cd., Kadikoy, Istanbul, Turkey
Medical Park Group, Istanbul

Emsey Hospital, Pendik, Istanbul
Çamlık, Selçuklu Cd. No:22, 34912 Pendik/İstanbul, Türkiye
Emsey Hospital, Pendik, Istanbul


American Hospital, Istanbul
Guzelbahce Sk. No:20, 34365, Nisantasi, Istanbul, Turkey
American Hospital, Istanbul

Memorial Hospitals Group
Burhaniye, Nagehan Sokağı No:4/A D:1, 34676 Üsküdar/İstanbul, Türkiye
Memorial Hospitals Group

Florence Nightingale Hospital Istanbul
Abide-i Hürriyet Cd No:166, 34381 Sisli, Istanbul
Florence Nightingale Hospital Istanbul

Medicana International Hospital, Istanbul
Halit Ziya Turkkani Mah. Medikal Park Cd. No:1, Beylikdüzü, İstanbul
Medicana International Hospital, Istanbul

Okan University Hospital Istanbul
Icmeler Mah. Aydınlıyolu Cd. No:2, 34947 Icmeler-Tuzla, Istanbul
Okan University Hospital Istanbul

Kolan International Hospital, Istanbul
Kaptanpasa Mah. Okmeydan Kavsagi, Darulaceze Cd. No:14, 34384 Sisli, Istanbul
Kolan International Hospital, Istanbul
Frequently Asked Questions
Get answers to common questions about medical tourism, treatment procedures, and our comprehensive healthcare services.
Ready To Start Your Healing Journey?
Get Personalized Medical Treatment Options From India's Top Hospitals. Our Medical Experts Are Ready To Assist You Every Step Of The Way.